Michael Chiu, Nivethika Jeyakumar, Graham Smith, Danielle M Nash, Mohamed Abou El Hassan, Dana Bailey, Peter Catomaris, Kika Veljkovic, Louise Moist, Amit X Garg, Arsh K Jain
{"title":"门诊高钾血症的频率、管理和结果:一项基于人群的队列研究。","authors":"Michael Chiu, Nivethika Jeyakumar, Graham Smith, Danielle M Nash, Mohamed Abou El Hassan, Dana Bailey, Peter Catomaris, Kika Veljkovic, Louise Moist, Amit X Garg, Arsh K Jain","doi":"10.1177/20543581251356568","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hyperkalemia is a potentially life-threatening condition, with guidelines recommending urgent treatment when the serum potassium level is greater than 6.0 mmol/L. However, these recommendations are inconsistent, leading to diverse approaches to patient care.</p><p><strong>Objectives: </strong>The primary objectives were to use population-based datasets to determine how often outpatient hyperkalemia (K > 6.2 mmol/L) occurs and how frequently patients present to the emergency department (ED) within 24 hours of the hyperkalemia report. Secondary objectives were to compare the characteristics of patients who had an ED encounter to those who did not, assess clinical outcomes within 7 days of the hyperkalemia report, and describe the initial potassium result within 24 hours of an ED encounter.</p><p><strong>Design: </strong>Retrospective cohort study using linked population-based datasets at ICES.</p><p><strong>Setting: </strong>Ontario, Canada from January 1, 2007, to December 24, 2021.</p><p><strong>Patients: </strong>Adult patients (≥18 years) not on dialysis with an outpatient hyperkalemia result >6.2 mmol/L who were identified through flagged and urgently communicated results from outpatient laboratories.</p><p><strong>Measurements: </strong>Emergency department encounters within 24 hours following an outpatient serum potassium report >6.2 mmol/L. Outcomes included all-cause mortality, cardiovascular mortality, arrhythmias, cardiac arrest in the ED, hospitalizations, and new dialysis starts within 7 days of the hyperkalemia report.</p><p><strong>Methods: </strong>Administrative healthcare data were linked with laboratory results to compare baseline characteristics, medication use, healthcare utilization, and clinical outcomes for all patients. Standardized differences were used for comparisons.</p><p><strong>Results: </strong>There were over 65 million serum potassium measurements and 57 607 individuals with an outpatient hyperkalemia value >6.2 mmol/L. Of these, 7469 (13.0%) individuals had an ED encounter within 24 hours. Individuals with an ED encounter had more comorbidities, higher medication use, and more prior healthcare utilization. Within 7 days of the hyperkalemia report, 675 of the 57 607 individuals (1.2%) had died. Where data were available, the first potassium value within 24 hours of an ED encounter was 1.5 mmol/L (± SD 1.3) lower, on average, than the initial outpatient potassium value.</p><p><strong>Limitations: </strong>All-cause mortality may not be attributable to the hyperkalemia result. Sudden cardiac death, which is more specific to hyperkalemia, is not completely captured in our data sources. Data for medications are limited to patients 65 years of age and older.</p><p><strong>Conclusions: </strong>Outpatient hyperkalemia is common. Despite guidelines recommending urgent treatment for patients with serum potassium levels >6.2 mmol/L, most are not referred to the ED.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251356568"},"PeriodicalIF":1.5000,"publicationDate":"2025-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317165/pdf/","citationCount":"0","resultStr":"{\"title\":\"Frequency, Management, and Outcomes of Outpatient Hyperkalemia: A Population-Based Cohort Study.\",\"authors\":\"Michael Chiu, Nivethika Jeyakumar, Graham Smith, Danielle M Nash, Mohamed Abou El Hassan, Dana Bailey, Peter Catomaris, Kika Veljkovic, Louise Moist, Amit X Garg, Arsh K Jain\",\"doi\":\"10.1177/20543581251356568\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hyperkalemia is a potentially life-threatening condition, with guidelines recommending urgent treatment when the serum potassium level is greater than 6.0 mmol/L. However, these recommendations are inconsistent, leading to diverse approaches to patient care.</p><p><strong>Objectives: </strong>The primary objectives were to use population-based datasets to determine how often outpatient hyperkalemia (K > 6.2 mmol/L) occurs and how frequently patients present to the emergency department (ED) within 24 hours of the hyperkalemia report. Secondary objectives were to compare the characteristics of patients who had an ED encounter to those who did not, assess clinical outcomes within 7 days of the hyperkalemia report, and describe the initial potassium result within 24 hours of an ED encounter.</p><p><strong>Design: </strong>Retrospective cohort study using linked population-based datasets at ICES.</p><p><strong>Setting: </strong>Ontario, Canada from January 1, 2007, to December 24, 2021.</p><p><strong>Patients: </strong>Adult patients (≥18 years) not on dialysis with an outpatient hyperkalemia result >6.2 mmol/L who were identified through flagged and urgently communicated results from outpatient laboratories.</p><p><strong>Measurements: </strong>Emergency department encounters within 24 hours following an outpatient serum potassium report >6.2 mmol/L. Outcomes included all-cause mortality, cardiovascular mortality, arrhythmias, cardiac arrest in the ED, hospitalizations, and new dialysis starts within 7 days of the hyperkalemia report.</p><p><strong>Methods: </strong>Administrative healthcare data were linked with laboratory results to compare baseline characteristics, medication use, healthcare utilization, and clinical outcomes for all patients. Standardized differences were used for comparisons.</p><p><strong>Results: </strong>There were over 65 million serum potassium measurements and 57 607 individuals with an outpatient hyperkalemia value >6.2 mmol/L. Of these, 7469 (13.0%) individuals had an ED encounter within 24 hours. Individuals with an ED encounter had more comorbidities, higher medication use, and more prior healthcare utilization. Within 7 days of the hyperkalemia report, 675 of the 57 607 individuals (1.2%) had died. Where data were available, the first potassium value within 24 hours of an ED encounter was 1.5 mmol/L (± SD 1.3) lower, on average, than the initial outpatient potassium value.</p><p><strong>Limitations: </strong>All-cause mortality may not be attributable to the hyperkalemia result. Sudden cardiac death, which is more specific to hyperkalemia, is not completely captured in our data sources. Data for medications are limited to patients 65 years of age and older.</p><p><strong>Conclusions: </strong>Outpatient hyperkalemia is common. Despite guidelines recommending urgent treatment for patients with serum potassium levels >6.2 mmol/L, most are not referred to the ED.</p>\",\"PeriodicalId\":9426,\"journal\":{\"name\":\"Canadian Journal of Kidney Health and Disease\",\"volume\":\"12 \",\"pages\":\"20543581251356568\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-07-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317165/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Kidney Health and Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20543581251356568\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251356568","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Frequency, Management, and Outcomes of Outpatient Hyperkalemia: A Population-Based Cohort Study.
Background: Hyperkalemia is a potentially life-threatening condition, with guidelines recommending urgent treatment when the serum potassium level is greater than 6.0 mmol/L. However, these recommendations are inconsistent, leading to diverse approaches to patient care.
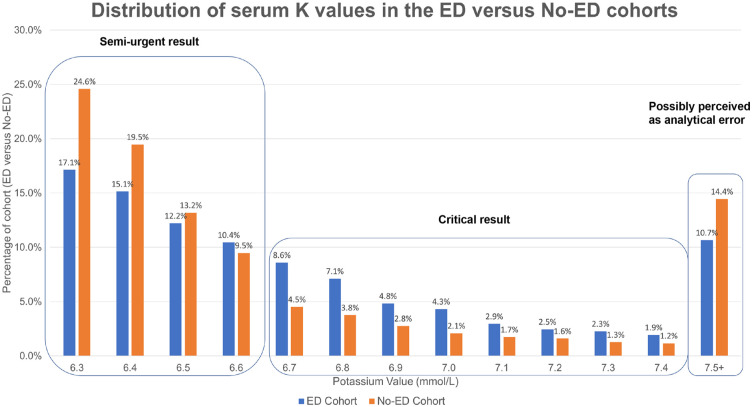
Objectives: The primary objectives were to use population-based datasets to determine how often outpatient hyperkalemia (K > 6.2 mmol/L) occurs and how frequently patients present to the emergency department (ED) within 24 hours of the hyperkalemia report. Secondary objectives were to compare the characteristics of patients who had an ED encounter to those who did not, assess clinical outcomes within 7 days of the hyperkalemia report, and describe the initial potassium result within 24 hours of an ED encounter.
Design: Retrospective cohort study using linked population-based datasets at ICES.
Setting: Ontario, Canada from January 1, 2007, to December 24, 2021.
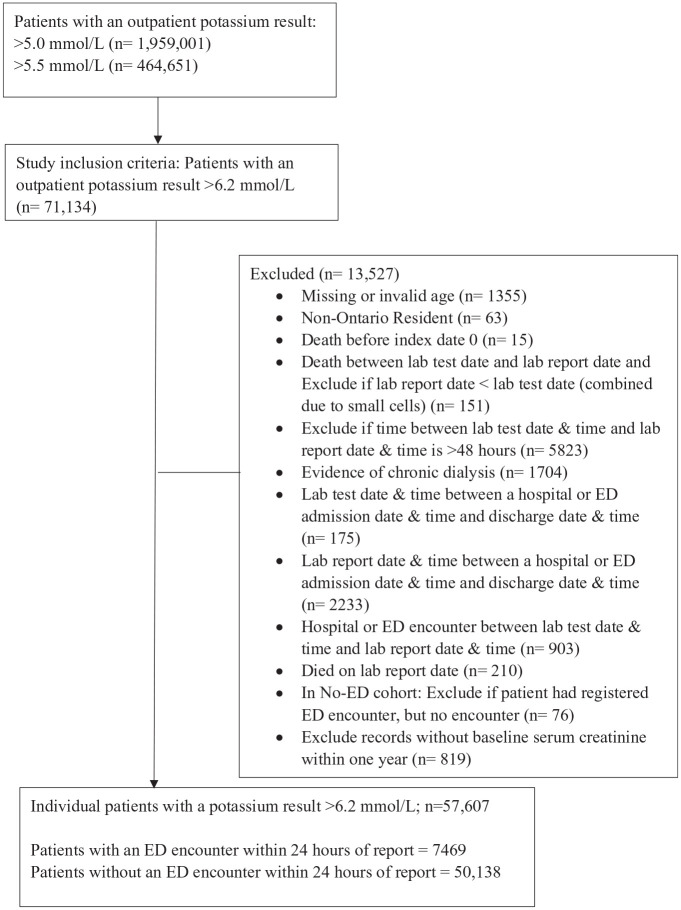
Patients: Adult patients (≥18 years) not on dialysis with an outpatient hyperkalemia result >6.2 mmol/L who were identified through flagged and urgently communicated results from outpatient laboratories.
Measurements: Emergency department encounters within 24 hours following an outpatient serum potassium report >6.2 mmol/L. Outcomes included all-cause mortality, cardiovascular mortality, arrhythmias, cardiac arrest in the ED, hospitalizations, and new dialysis starts within 7 days of the hyperkalemia report.
Methods: Administrative healthcare data were linked with laboratory results to compare baseline characteristics, medication use, healthcare utilization, and clinical outcomes for all patients. Standardized differences were used for comparisons.
Results: There were over 65 million serum potassium measurements and 57 607 individuals with an outpatient hyperkalemia value >6.2 mmol/L. Of these, 7469 (13.0%) individuals had an ED encounter within 24 hours. Individuals with an ED encounter had more comorbidities, higher medication use, and more prior healthcare utilization. Within 7 days of the hyperkalemia report, 675 of the 57 607 individuals (1.2%) had died. Where data were available, the first potassium value within 24 hours of an ED encounter was 1.5 mmol/L (± SD 1.3) lower, on average, than the initial outpatient potassium value.
Limitations: All-cause mortality may not be attributable to the hyperkalemia result. Sudden cardiac death, which is more specific to hyperkalemia, is not completely captured in our data sources. Data for medications are limited to patients 65 years of age and older.
Conclusions: Outpatient hyperkalemia is common. Despite guidelines recommending urgent treatment for patients with serum potassium levels >6.2 mmol/L, most are not referred to the ED.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


