Ana Muñoz-Sánchez, Leyre Martín-Rodríguez, Paula López-Sánchez, Maria Valdenebro, Maria Luisa Serrano-Salazar, Maria Marques, Jose Portoles
{"title":"公共卫生系统的中期和长期AKI结果。","authors":"Ana Muñoz-Sánchez, Leyre Martín-Rodríguez, Paula López-Sánchez, Maria Valdenebro, Maria Luisa Serrano-Salazar, Maria Marques, Jose Portoles","doi":"10.1007/s40620-025-02367-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute Kidney Injury (AKI) is frequent and is associated with adverse outcomes.</p><p><strong>Aims: </strong>To analyze the impact of community-acquired and hospital-acquired AKI on in-hospital and five-year post-discharge kidney replacement therapy (KRT) requirement in the pre-COVID era.</p><p><strong>Methods: </strong>We linked the regional health system database of 419,851 admissions to the regional KRT registry. We grouped all admissions into 3 categories: community-acquired AKI, where AKI was the primary diagnosis, and hospital-acquired AKI, where AKI was an additional diagnosis alongside another primary condition. Admissions without this code were grouped into a third category (no AKI). We excluded patients aged under 18 years old, those with previous KRT, and pregnant women. The study was approved by the ethics committee. Patients were followed up for five years after discharge.</p><p><strong>Results: </strong>Community-acquired AKI accounted for 0.6% of all admissions, associated prolonged average hospital stays, and increased mortality rates. In-hospital KRT administration was required in 3.1% of cases, and after a mean follow-up time of 459 days, 7.2% of these patients began chronic KRT. Hospital-acquired AKI represented 6.1% of all admissions and was associated with the highest mortality rate (22.9% vs 14.4% in the community-acquired AKI group) and the longest average hospital stay (12.6 days vs 7.1 in the no AKI group). Only 0.5% of hospital-acquired AKI cases required KRT during the AKI episode, while 2% of these patients initiated chronic KRT after a mean follow-up time of 594 days.</p><p><strong>Conclusions: </strong>AKI continues to be a frequent problem in clinical practice, negatively influencing patient morbidity and mortality, and increasing the risk of starting KRT in the medium-long term.</p>","PeriodicalId":16542,"journal":{"name":"Journal of Nephrology","volume":" ","pages":"1985-1994"},"PeriodicalIF":2.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12484351/pdf/","citationCount":"0","resultStr":"{\"title\":\"Intermediate and long-term AKI outcomes in a public health system.\",\"authors\":\"Ana Muñoz-Sánchez, Leyre Martín-Rodríguez, Paula López-Sánchez, Maria Valdenebro, Maria Luisa Serrano-Salazar, Maria Marques, Jose Portoles\",\"doi\":\"10.1007/s40620-025-02367-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute Kidney Injury (AKI) is frequent and is associated with adverse outcomes.</p><p><strong>Aims: </strong>To analyze the impact of community-acquired and hospital-acquired AKI on in-hospital and five-year post-discharge kidney replacement therapy (KRT) requirement in the pre-COVID era.</p><p><strong>Methods: </strong>We linked the regional health system database of 419,851 admissions to the regional KRT registry. We grouped all admissions into 3 categories: community-acquired AKI, where AKI was the primary diagnosis, and hospital-acquired AKI, where AKI was an additional diagnosis alongside another primary condition. Admissions without this code were grouped into a third category (no AKI). We excluded patients aged under 18 years old, those with previous KRT, and pregnant women. The study was approved by the ethics committee. Patients were followed up for five years after discharge.</p><p><strong>Results: </strong>Community-acquired AKI accounted for 0.6% of all admissions, associated prolonged average hospital stays, and increased mortality rates. In-hospital KRT administration was required in 3.1% of cases, and after a mean follow-up time of 459 days, 7.2% of these patients began chronic KRT. Hospital-acquired AKI represented 6.1% of all admissions and was associated with the highest mortality rate (22.9% vs 14.4% in the community-acquired AKI group) and the longest average hospital stay (12.6 days vs 7.1 in the no AKI group). Only 0.5% of hospital-acquired AKI cases required KRT during the AKI episode, while 2% of these patients initiated chronic KRT after a mean follow-up time of 594 days.</p><p><strong>Conclusions: </strong>AKI continues to be a frequent problem in clinical practice, negatively influencing patient morbidity and mortality, and increasing the risk of starting KRT in the medium-long term.</p>\",\"PeriodicalId\":16542,\"journal\":{\"name\":\"Journal of Nephrology\",\"volume\":\" \",\"pages\":\"1985-1994\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12484351/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Nephrology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40620-025-02367-6\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Nephrology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40620-025-02367-6","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:急性肾损伤(AKI)是一种常见的疾病,并伴有不良后果。目的:分析社区获得性和医院获得性AKI对新冠肺炎前住院和出院后5年肾脏替代治疗(KRT)需求的影响。方法:我们将419,851名入院患者的区域卫生系统数据库与区域KRT登记处联系起来。我们将所有入院患者分为3类:社区获得性AKI,其中AKI是主要诊断;医院获得性AKI,其中AKI是另一种主要疾病的附加诊断。没有此代码的录取被归为第三类(无AKI)。我们排除了18岁以下的患者、既往KRT患者和孕妇。这项研究得到了伦理委员会的批准。出院后随访5年。结果:社区获得性AKI占所有入院人数的0.6%,相关的平均住院时间延长,死亡率增加。3.1%的病例需要住院KRT治疗,平均随访459天后,这些患者中有7.2%开始慢性KRT治疗。医院获得性AKI占所有住院患者的6.1%,死亡率最高(22.9% vs 14.4%),平均住院时间最长(12.6天vs 7.1天,无AKI组)。只有0.5%的医院获得性AKI病例在AKI发作期间需要KRT,而这些患者中有2%在平均随访594天后开始慢性KRT。结论:AKI在临床实践中仍然是一个常见的问题,对患者的发病率和死亡率产生负面影响,并且在中长期内增加了开始KRT的风险。
Intermediate and long-term AKI outcomes in a public health system.
Background: Acute Kidney Injury (AKI) is frequent and is associated with adverse outcomes.
Aims: To analyze the impact of community-acquired and hospital-acquired AKI on in-hospital and five-year post-discharge kidney replacement therapy (KRT) requirement in the pre-COVID era.
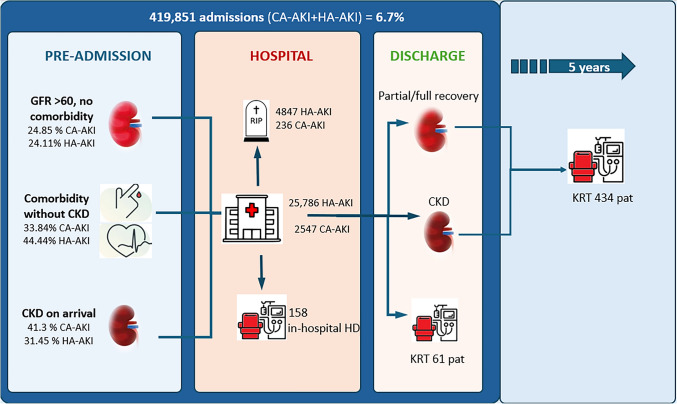
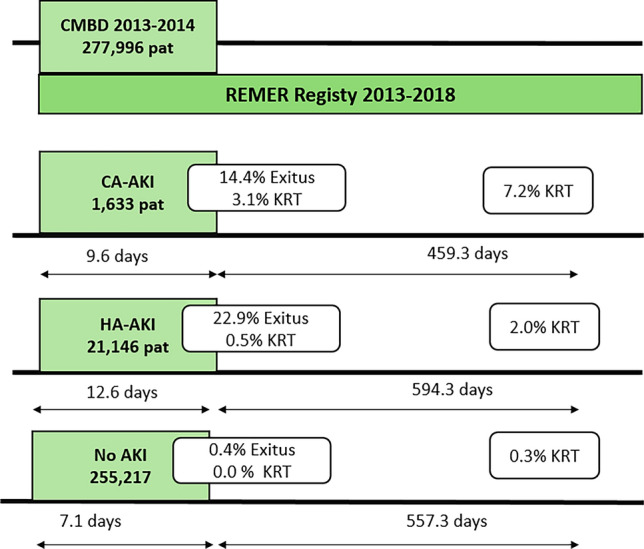
Methods: We linked the regional health system database of 419,851 admissions to the regional KRT registry. We grouped all admissions into 3 categories: community-acquired AKI, where AKI was the primary diagnosis, and hospital-acquired AKI, where AKI was an additional diagnosis alongside another primary condition. Admissions without this code were grouped into a third category (no AKI). We excluded patients aged under 18 years old, those with previous KRT, and pregnant women. The study was approved by the ethics committee. Patients were followed up for five years after discharge.
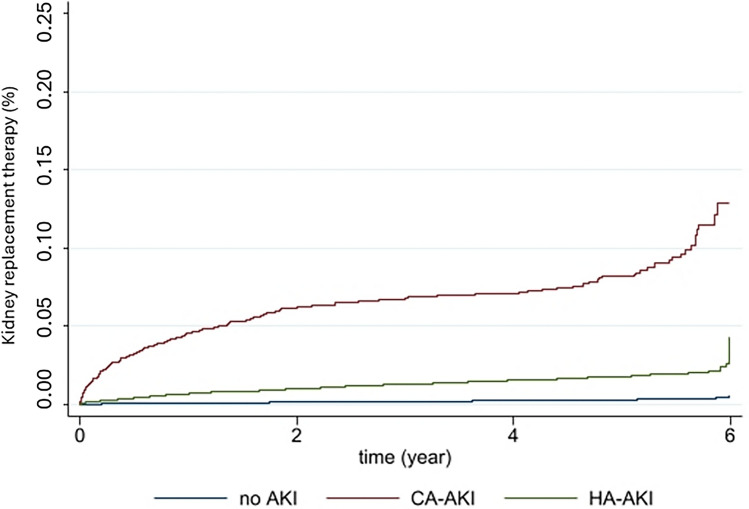
Results: Community-acquired AKI accounted for 0.6% of all admissions, associated prolonged average hospital stays, and increased mortality rates. In-hospital KRT administration was required in 3.1% of cases, and after a mean follow-up time of 459 days, 7.2% of these patients began chronic KRT. Hospital-acquired AKI represented 6.1% of all admissions and was associated with the highest mortality rate (22.9% vs 14.4% in the community-acquired AKI group) and the longest average hospital stay (12.6 days vs 7.1 in the no AKI group). Only 0.5% of hospital-acquired AKI cases required KRT during the AKI episode, while 2% of these patients initiated chronic KRT after a mean follow-up time of 594 days.
Conclusions: AKI continues to be a frequent problem in clinical practice, negatively influencing patient morbidity and mortality, and increasing the risk of starting KRT in the medium-long term.
期刊介绍:
Journal of Nephrology is a bimonthly journal that considers publication of peer reviewed original manuscripts dealing with both clinical and laboratory investigations of relevance to the broad fields of Nephrology, Dialysis and Transplantation. It is the Official Journal of the Italian Society of Nephrology (SIN).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


