Thabuna Sivaprakasam, Prachaya Nitchaikulvatana, Jodi Gedallovich, Jagruti Shah, Matthew Charles Baker
{"title":"免疫检查点抑制剂治疗后转移性黑色素瘤患者发生igg4相关疾病伴间质性肾炎:1例报告","authors":"Thabuna Sivaprakasam, Prachaya Nitchaikulvatana, Jodi Gedallovich, Jagruti Shah, Matthew Charles Baker","doi":"10.1186/s41927-025-00548-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Immune checkpoint inhibitors (ICIs) have become a cornerstone in the treatment of metastatic melanoma. Several case reports have documented IgG4-related disease (IgG4-RD) as an adverse event following ICI therapy. Here we report the first instance of interstitial nephritis associated with IgG4-RD as an immune-related adverse event (irAE) following ICI treatment.</p><p><strong>Case presentation: </strong>A 71-year-old male with malignant melanoma (BRAF wild-type) initially received one cycle of adjuvant pembrolizumab, followed by four cycles of ipilimumab/nivolumab after the occurrence of lung metastases. Four months later, a follow-up computed tomography (CT) revealed infiltrative masses in the kidneys, along with abnormal mediastinal and hilar lymphadenopathy but his baseline serum creatinine remained stable. A subsequent kidney biopsy showed renal parenchyma with significant interstitial nephritis and an increase in IgG4-positive plasma cells, with no evidence of malignancy. Plasma IgG4 levels were elevated at 294 mg/dL (normal 11-157 mg/dL), and complement C4 level was low at < 8 mg/dL. In addition, the patient had an asymptomatic rise in lipase (105 U/L, normal 7-60 U/L), but had no other findings to suggest pancreatitis. The patient was started on prednisone 40 mg daily with a plan to taper. A follow-up CT scan performed four weeks later showed near-complete resolution of the previously observed mediastinal lymphadenopathy and bilateral infiltrative renal masses.</p><p><strong>Conclusion: </strong>This represents the first reported case of interstitial nephritis resulting from IgG4-related disease following ICI treatment. Clinicians should consider the potential for IgG4-RD, particularly with associated renal manifestations, in patients undergoing ICI therapy. Early recognition and treatment of this rare side effect can significantly impact the clinical outcome. This case highlights the importance of being vigilant for uncommon and new adverse effects following ICI treatment, especially as the field continues to evolve and new immunotherapies are developed.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>","PeriodicalId":9150,"journal":{"name":"BMC Rheumatology","volume":"9 1","pages":"95"},"PeriodicalIF":2.5000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12315461/pdf/","citationCount":"0","resultStr":"{\"title\":\"IgG4-related disease with interstitial nephritis in a patient with metastatic melanoma following immune checkpoint inhibitor treatment: a case report.\",\"authors\":\"Thabuna Sivaprakasam, Prachaya Nitchaikulvatana, Jodi Gedallovich, Jagruti Shah, Matthew Charles Baker\",\"doi\":\"10.1186/s41927-025-00548-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Immune checkpoint inhibitors (ICIs) have become a cornerstone in the treatment of metastatic melanoma. Several case reports have documented IgG4-related disease (IgG4-RD) as an adverse event following ICI therapy. Here we report the first instance of interstitial nephritis associated with IgG4-RD as an immune-related adverse event (irAE) following ICI treatment.</p><p><strong>Case presentation: </strong>A 71-year-old male with malignant melanoma (BRAF wild-type) initially received one cycle of adjuvant pembrolizumab, followed by four cycles of ipilimumab/nivolumab after the occurrence of lung metastases. Four months later, a follow-up computed tomography (CT) revealed infiltrative masses in the kidneys, along with abnormal mediastinal and hilar lymphadenopathy but his baseline serum creatinine remained stable. A subsequent kidney biopsy showed renal parenchyma with significant interstitial nephritis and an increase in IgG4-positive plasma cells, with no evidence of malignancy. Plasma IgG4 levels were elevated at 294 mg/dL (normal 11-157 mg/dL), and complement C4 level was low at < 8 mg/dL. In addition, the patient had an asymptomatic rise in lipase (105 U/L, normal 7-60 U/L), but had no other findings to suggest pancreatitis. The patient was started on prednisone 40 mg daily with a plan to taper. A follow-up CT scan performed four weeks later showed near-complete resolution of the previously observed mediastinal lymphadenopathy and bilateral infiltrative renal masses.</p><p><strong>Conclusion: </strong>This represents the first reported case of interstitial nephritis resulting from IgG4-related disease following ICI treatment. Clinicians should consider the potential for IgG4-RD, particularly with associated renal manifestations, in patients undergoing ICI therapy. Early recognition and treatment of this rare side effect can significantly impact the clinical outcome. This case highlights the importance of being vigilant for uncommon and new adverse effects following ICI treatment, especially as the field continues to evolve and new immunotherapies are developed.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>\",\"PeriodicalId\":9150,\"journal\":{\"name\":\"BMC Rheumatology\",\"volume\":\"9 1\",\"pages\":\"95\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12315461/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41927-025-00548-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41927-025-00548-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
IgG4-related disease with interstitial nephritis in a patient with metastatic melanoma following immune checkpoint inhibitor treatment: a case report.
Background: Immune checkpoint inhibitors (ICIs) have become a cornerstone in the treatment of metastatic melanoma. Several case reports have documented IgG4-related disease (IgG4-RD) as an adverse event following ICI therapy. Here we report the first instance of interstitial nephritis associated with IgG4-RD as an immune-related adverse event (irAE) following ICI treatment.
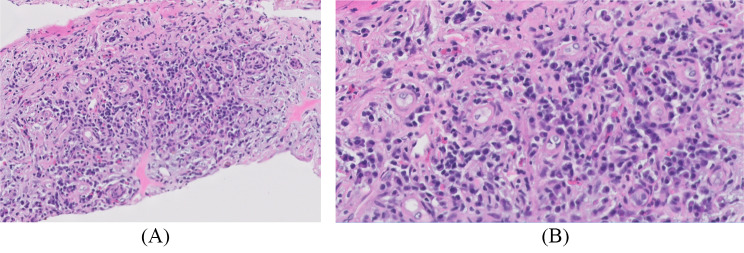
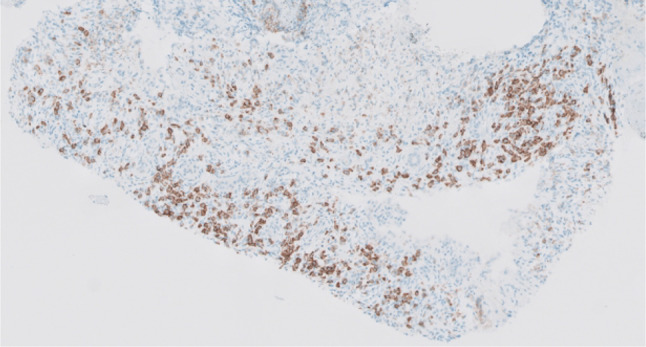
Case presentation: A 71-year-old male with malignant melanoma (BRAF wild-type) initially received one cycle of adjuvant pembrolizumab, followed by four cycles of ipilimumab/nivolumab after the occurrence of lung metastases. Four months later, a follow-up computed tomography (CT) revealed infiltrative masses in the kidneys, along with abnormal mediastinal and hilar lymphadenopathy but his baseline serum creatinine remained stable. A subsequent kidney biopsy showed renal parenchyma with significant interstitial nephritis and an increase in IgG4-positive plasma cells, with no evidence of malignancy. Plasma IgG4 levels were elevated at 294 mg/dL (normal 11-157 mg/dL), and complement C4 level was low at < 8 mg/dL. In addition, the patient had an asymptomatic rise in lipase (105 U/L, normal 7-60 U/L), but had no other findings to suggest pancreatitis. The patient was started on prednisone 40 mg daily with a plan to taper. A follow-up CT scan performed four weeks later showed near-complete resolution of the previously observed mediastinal lymphadenopathy and bilateral infiltrative renal masses.
Conclusion: This represents the first reported case of interstitial nephritis resulting from IgG4-related disease following ICI treatment. Clinicians should consider the potential for IgG4-RD, particularly with associated renal manifestations, in patients undergoing ICI therapy. Early recognition and treatment of this rare side effect can significantly impact the clinical outcome. This case highlights the importance of being vigilant for uncommon and new adverse effects following ICI treatment, especially as the field continues to evolve and new immunotherapies are developed.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


