Pankaj Garg, Aradhai Bana, Gareth Matthews, Tiya Bali, Rui Li, Zia Mehmood, Liang Zhong, Rob J van der Geest, Sven Plein, John P Greenwood, Peter Swoboda
{"title":"心血管磁共振肺毛细血管楔压在急性心肌梗死中的血流动力学意义。","authors":"Pankaj Garg, Aradhai Bana, Gareth Matthews, Tiya Bali, Rui Li, Zia Mehmood, Liang Zhong, Rob J van der Geest, Sven Plein, John P Greenwood, Peter Swoboda","doi":"10.1093/ehjimp/qyaf086","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Cardiovascular magnetic resonance (CMR)-derived pulmonary capillary wedge pressure (PCWP) has demonstrated diagnostic and prognostic utility in heart failure patients. However, its clinical value in acute myocardial infarction (AMI) remains undetermined. This study investigates the relationship between CMR-derived PCWP, myocardial injury, and left ventricular (LV) remodelling in re-perfused acute ST-elevation myocardial infarction (STEMI).</p><p><strong>Methods and results: </strong>Sixty-nine patients with STEMI underwent CMR within 48 h and at 3 months. PCWP was estimated using the sex-specific equation: CMR PCWP: 5.7591 + (0.07505 × left atrial volume) [0.05289 × left ventricular mass (LVM)] - (1.9927 × sex) [female = 0; male = 1], where LAV is left atrial volume (mL) and LVM is left ventricular mass (g). LV remodelling was assessed via changes in LV end-diastolic volume (LVEDV) and ejection fraction (LVEF). Patients with high CMR PCWP (≥18 mmHg) exhibited greater myocardial scar burden (28.5% vs. 17.2%, <i>P</i> = 0.0008) and microvascular obstruction (7.6% vs. 2.5%, <i>P</i> < 0.0001). They also had higher acute LVEDV (193.7 ± 39.7 vs. 158.0 ± 29.5 mL, <i>P</i> < 0.0001) and lower LVEF (41.4 ± 10.4% vs. 48.5 ± 9.2%, <i>P</i> = 0.0066). At follow-up, higher baseline CMR PCWP was associated with greater LV remodelling (<i>P</i> < 0.0001) and persistently reduced LVEF (45.4 ± 10.2% vs. 55.0 ± 10.3%, <i>P</i> = 0.0005). Regression analysis confirmed baseline PCWP as an independent predictor of follow-up LVEF (<i>P</i> = 0.0036).</p><p><strong>Conclusion: </strong>CMR-derived PCWP may be a valuable biomarker in STEMI, identifying patients at risk of adverse remodelling and LV dysfunction. Its integration into clinical practice may enhance risk stratification and guide targeted therapies.</p>","PeriodicalId":94317,"journal":{"name":"European heart journal. Imaging methods and practice","volume":"3 2","pages":"qyaf086"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12311366/pdf/","citationCount":"0","resultStr":"{\"title\":\"Haemodynamic implications of cardiovascular magnetic resonance pulmonary capillary wedge pressure in acute myocardial infarction.\",\"authors\":\"Pankaj Garg, Aradhai Bana, Gareth Matthews, Tiya Bali, Rui Li, Zia Mehmood, Liang Zhong, Rob J van der Geest, Sven Plein, John P Greenwood, Peter Swoboda\",\"doi\":\"10.1093/ehjimp/qyaf086\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Cardiovascular magnetic resonance (CMR)-derived pulmonary capillary wedge pressure (PCWP) has demonstrated diagnostic and prognostic utility in heart failure patients. However, its clinical value in acute myocardial infarction (AMI) remains undetermined. This study investigates the relationship between CMR-derived PCWP, myocardial injury, and left ventricular (LV) remodelling in re-perfused acute ST-elevation myocardial infarction (STEMI).</p><p><strong>Methods and results: </strong>Sixty-nine patients with STEMI underwent CMR within 48 h and at 3 months. PCWP was estimated using the sex-specific equation: CMR PCWP: 5.7591 + (0.07505 × left atrial volume) [0.05289 × left ventricular mass (LVM)] - (1.9927 × sex) [female = 0; male = 1], where LAV is left atrial volume (mL) and LVM is left ventricular mass (g). LV remodelling was assessed via changes in LV end-diastolic volume (LVEDV) and ejection fraction (LVEF). Patients with high CMR PCWP (≥18 mmHg) exhibited greater myocardial scar burden (28.5% vs. 17.2%, <i>P</i> = 0.0008) and microvascular obstruction (7.6% vs. 2.5%, <i>P</i> < 0.0001). They also had higher acute LVEDV (193.7 ± 39.7 vs. 158.0 ± 29.5 mL, <i>P</i> < 0.0001) and lower LVEF (41.4 ± 10.4% vs. 48.5 ± 9.2%, <i>P</i> = 0.0066). At follow-up, higher baseline CMR PCWP was associated with greater LV remodelling (<i>P</i> < 0.0001) and persistently reduced LVEF (45.4 ± 10.2% vs. 55.0 ± 10.3%, <i>P</i> = 0.0005). Regression analysis confirmed baseline PCWP as an independent predictor of follow-up LVEF (<i>P</i> = 0.0036).</p><p><strong>Conclusion: </strong>CMR-derived PCWP may be a valuable biomarker in STEMI, identifying patients at risk of adverse remodelling and LV dysfunction. Its integration into clinical practice may enhance risk stratification and guide targeted therapies.</p>\",\"PeriodicalId\":94317,\"journal\":{\"name\":\"European heart journal. Imaging methods and practice\",\"volume\":\"3 2\",\"pages\":\"qyaf086\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12311366/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal. Imaging methods and practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjimp/qyaf086\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Imaging methods and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjimp/qyaf086","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:心血管磁共振(CMR)衍生的肺毛细血管楔压(PCWP)在心力衰竭患者中的诊断和预后应用已被证实。然而,其在急性心肌梗死(AMI)中的临床价值尚未确定。本研究探讨再灌注急性st段抬高型心肌梗死(STEMI) cmr衍生的PCWP、心肌损伤和左室(LV)重构之间的关系。方法和结果:69例STEMI患者分别在48 h和3个月内行CMR。使用性别特异性方程估计PCWP: CMR PCWP: 5.7591 + (0.07505 ×左心房容积)[0.05289 ×左心室质量(LVM)] - (1.9927 ×性别)[女性= 0;male = 1],其中LAV为左心房容积(mL), LVM为左心室质量(g)。通过左室舒张末期容积(LVEDV)和射血分数(LVEF)的变化来评估左室重构。高CMR PCWP(≥18 mmHg)患者表现出更大的心肌疤痕负担(28.5% vs. 17.2%, P = 0.0008)和微血管阻塞(7.6% vs. 2.5%, P < 0.0001)。急性LVEDV升高(193.7±39.7 vs 158.0±29.5 mL, P < 0.0001), LVEF降低(41.4±10.4% vs 48.5±9.2%,P = 0.0066)。在随访中,较高的基线CMR PCWP与更大的左室重构(P < 0.0001)和持续降低的LVEF相关(45.4±10.2% vs. 55.0±10.3%,P = 0.0005)。回归分析证实基线PCWP是随访LVEF的独立预测因子(P = 0.0036)。结论:cmr衍生的PCWP可能是STEMI中有价值的生物标志物,可识别有不良重构和左室功能障碍风险的患者。将其纳入临床实践可加强风险分层,指导靶向治疗。
Haemodynamic implications of cardiovascular magnetic resonance pulmonary capillary wedge pressure in acute myocardial infarction.
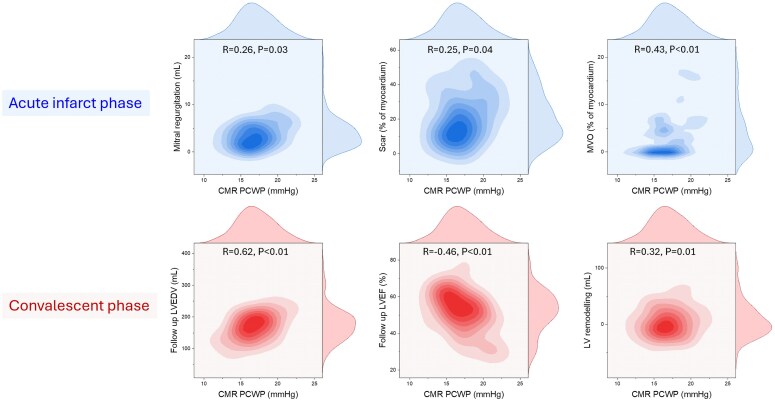
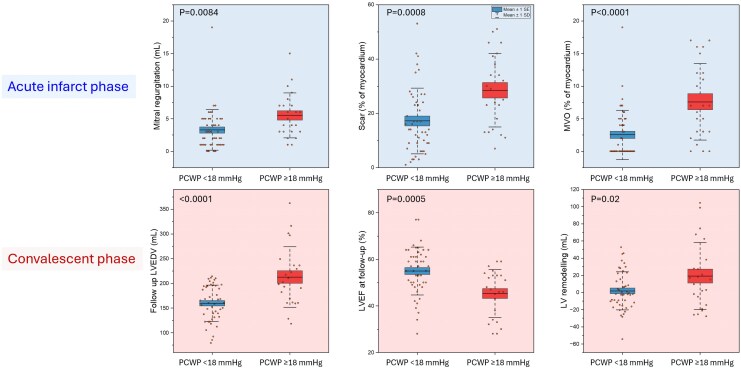
Aims: Cardiovascular magnetic resonance (CMR)-derived pulmonary capillary wedge pressure (PCWP) has demonstrated diagnostic and prognostic utility in heart failure patients. However, its clinical value in acute myocardial infarction (AMI) remains undetermined. This study investigates the relationship between CMR-derived PCWP, myocardial injury, and left ventricular (LV) remodelling in re-perfused acute ST-elevation myocardial infarction (STEMI).
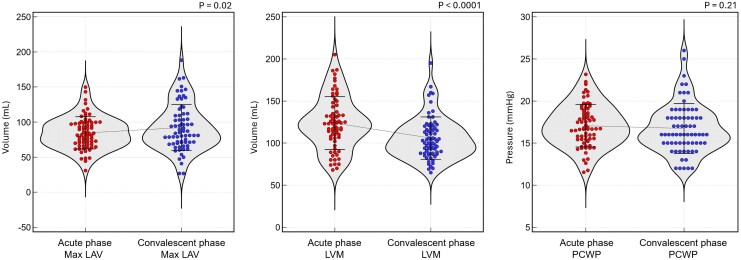
Methods and results: Sixty-nine patients with STEMI underwent CMR within 48 h and at 3 months. PCWP was estimated using the sex-specific equation: CMR PCWP: 5.7591 + (0.07505 × left atrial volume) [0.05289 × left ventricular mass (LVM)] - (1.9927 × sex) [female = 0; male = 1], where LAV is left atrial volume (mL) and LVM is left ventricular mass (g). LV remodelling was assessed via changes in LV end-diastolic volume (LVEDV) and ejection fraction (LVEF). Patients with high CMR PCWP (≥18 mmHg) exhibited greater myocardial scar burden (28.5% vs. 17.2%, P = 0.0008) and microvascular obstruction (7.6% vs. 2.5%, P < 0.0001). They also had higher acute LVEDV (193.7 ± 39.7 vs. 158.0 ± 29.5 mL, P < 0.0001) and lower LVEF (41.4 ± 10.4% vs. 48.5 ± 9.2%, P = 0.0066). At follow-up, higher baseline CMR PCWP was associated with greater LV remodelling (P < 0.0001) and persistently reduced LVEF (45.4 ± 10.2% vs. 55.0 ± 10.3%, P = 0.0005). Regression analysis confirmed baseline PCWP as an independent predictor of follow-up LVEF (P = 0.0036).
Conclusion: CMR-derived PCWP may be a valuable biomarker in STEMI, identifying patients at risk of adverse remodelling and LV dysfunction. Its integration into clinical practice may enhance risk stratification and guide targeted therapies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


