Carolin Jung, Andre Gerdes, Hans-Joerg Gillmann, Thomas Stueber
{"title":"术前常规咪达唑仑处方的遗漏与术前交感神经激活增加有关,但与死亡率无关:倾向评分匹配,前后研究。","authors":"Carolin Jung, Andre Gerdes, Hans-Joerg Gillmann, Thomas Stueber","doi":"10.1186/s13741-025-00568-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Guidelines recommend avoiding preoperative anxiolytic medication with midazolam. However, the risk-benefit ratio of preoperative midazolam prescriptions remains unclear. This study aimed to investigate the association between preoperative midazolam prescription and perioperative in-house mortality as well as preoperative cardiovascular stress.</p><p><strong>Methods: </strong>We performed a retrospective single-center propensity score-matched study in a university hospital in Germany before and after de-implementation of routine oral preoperative midazolam prescription in December 2018. We included adult patients who underwent general anesthesia between December 1, 2017, and November 31, 2019. Patients who received midazolam premedication before de-implementation were compared to those who did not receive midazolam after de-implementation. After propensity score matching, we estimated the treatment effects using regression modeling. The primary endpoint was inhospital mortality after general surgery. Secondary endpoints included pre-induction vital signs, duration of stay in the postanesthesia care unit, and medications administered.</p><p><strong>Results: </strong>After propensity score matching, we analyzed 7421 patients in each group. In this adjusted analysis, premedication with midazolam was not associated with mortality (OR 0.91, 95% CI 0.60 to 1.38, p = 0.662). Midazolam premedication was associated with significantly lower pre-induction blood pressures, with an estimated average treatment effect for systolic blood pressure of - 5.33 mmHg (SE 0.41, 95% CI - 6.13 to - 4.52 mmHg).</p><p><strong>Conclusions: </strong>Midazolam prescription was not associated with increased mortality in a large cohort of surgical patients but with a lower pre-induction blood pressure and heart rate, suggesting a potential reduction in cardiovascular stress.</p>","PeriodicalId":19764,"journal":{"name":"Perioperative Medicine","volume":"14 1","pages":"81"},"PeriodicalIF":2.1000,"publicationDate":"2025-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12308930/pdf/","citationCount":"0","resultStr":"{\"title\":\"The omission of routine preoperative midazolam prescription is associated with increased preoperative sympathetic activation but not mortality: a propensity score matched, before-and-after study.\",\"authors\":\"Carolin Jung, Andre Gerdes, Hans-Joerg Gillmann, Thomas Stueber\",\"doi\":\"10.1186/s13741-025-00568-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Guidelines recommend avoiding preoperative anxiolytic medication with midazolam. However, the risk-benefit ratio of preoperative midazolam prescriptions remains unclear. This study aimed to investigate the association between preoperative midazolam prescription and perioperative in-house mortality as well as preoperative cardiovascular stress.</p><p><strong>Methods: </strong>We performed a retrospective single-center propensity score-matched study in a university hospital in Germany before and after de-implementation of routine oral preoperative midazolam prescription in December 2018. We included adult patients who underwent general anesthesia between December 1, 2017, and November 31, 2019. Patients who received midazolam premedication before de-implementation were compared to those who did not receive midazolam after de-implementation. After propensity score matching, we estimated the treatment effects using regression modeling. The primary endpoint was inhospital mortality after general surgery. Secondary endpoints included pre-induction vital signs, duration of stay in the postanesthesia care unit, and medications administered.</p><p><strong>Results: </strong>After propensity score matching, we analyzed 7421 patients in each group. In this adjusted analysis, premedication with midazolam was not associated with mortality (OR 0.91, 95% CI 0.60 to 1.38, p = 0.662). Midazolam premedication was associated with significantly lower pre-induction blood pressures, with an estimated average treatment effect for systolic blood pressure of - 5.33 mmHg (SE 0.41, 95% CI - 6.13 to - 4.52 mmHg).</p><p><strong>Conclusions: </strong>Midazolam prescription was not associated with increased mortality in a large cohort of surgical patients but with a lower pre-induction blood pressure and heart rate, suggesting a potential reduction in cardiovascular stress.</p>\",\"PeriodicalId\":19764,\"journal\":{\"name\":\"Perioperative Medicine\",\"volume\":\"14 1\",\"pages\":\"81\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-07-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12308930/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Perioperative Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13741-025-00568-y\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Perioperative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13741-025-00568-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:指南建议术前避免使用咪达唑仑抗焦虑药物。然而,术前处方咪达唑仑的风险收益比尚不清楚。本研究旨在探讨术前咪达唑仑处方与围手术期住院死亡率以及术前心血管压力之间的关系。方法:我们于2018年12月在德国一家大学医院进行了回顾性单中心倾向评分匹配研究,该研究于术前常规口服咪达唑仑处方取消实施前后进行。我们纳入了2017年12月1日至2019年11月31日期间接受全身麻醉的成年患者。将去实施前接受咪达唑仑预用药的患者与去实施后未接受咪达唑仑的患者进行比较。在倾向评分匹配后,我们使用回归模型估计治疗效果。主要终点是普通手术后的住院死亡率。次要终点包括诱导前生命体征、麻醉后护理病房的住院时间和用药情况。结果:经过倾向评分匹配,我们分析了每组7421例患者。在这个校正分析中,用药前使用咪达唑仑与死亡率无关(OR 0.91, 95% CI 0.60 ~ 1.38, p = 0.662)。咪达唑仑治疗前与诱导前血压显著降低相关,估计收缩压的平均治疗效果为- 5.33 mmHg (SE 0.41, 95% CI - 6.13至- 4.52 mmHg)。结论:在大量外科患者中,咪达唑仑处方与死亡率增加无关,但与诱导前血压和心率降低有关,提示可能降低心血管压力。
The omission of routine preoperative midazolam prescription is associated with increased preoperative sympathetic activation but not mortality: a propensity score matched, before-and-after study.
Background: Guidelines recommend avoiding preoperative anxiolytic medication with midazolam. However, the risk-benefit ratio of preoperative midazolam prescriptions remains unclear. This study aimed to investigate the association between preoperative midazolam prescription and perioperative in-house mortality as well as preoperative cardiovascular stress.
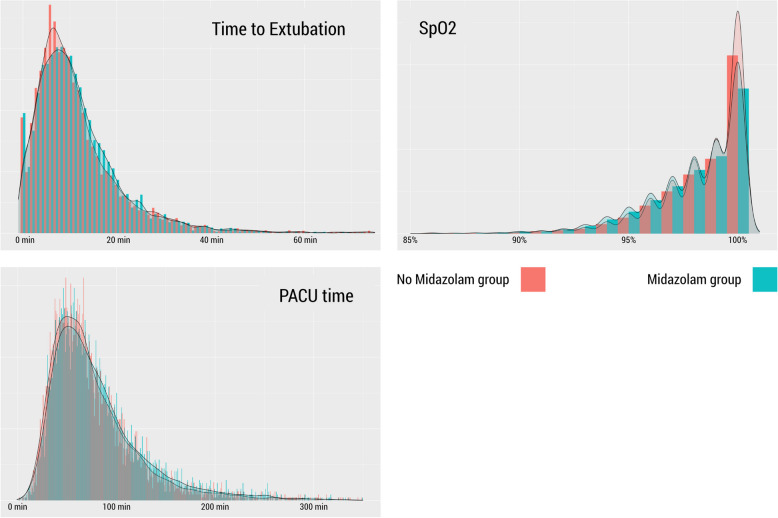
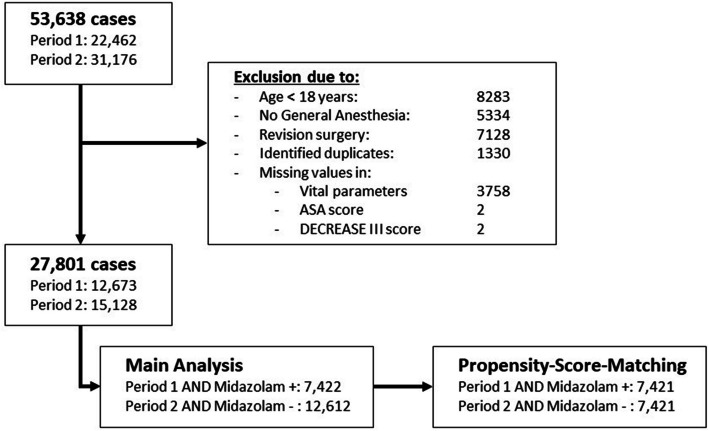
Methods: We performed a retrospective single-center propensity score-matched study in a university hospital in Germany before and after de-implementation of routine oral preoperative midazolam prescription in December 2018. We included adult patients who underwent general anesthesia between December 1, 2017, and November 31, 2019. Patients who received midazolam premedication before de-implementation were compared to those who did not receive midazolam after de-implementation. After propensity score matching, we estimated the treatment effects using regression modeling. The primary endpoint was inhospital mortality after general surgery. Secondary endpoints included pre-induction vital signs, duration of stay in the postanesthesia care unit, and medications administered.
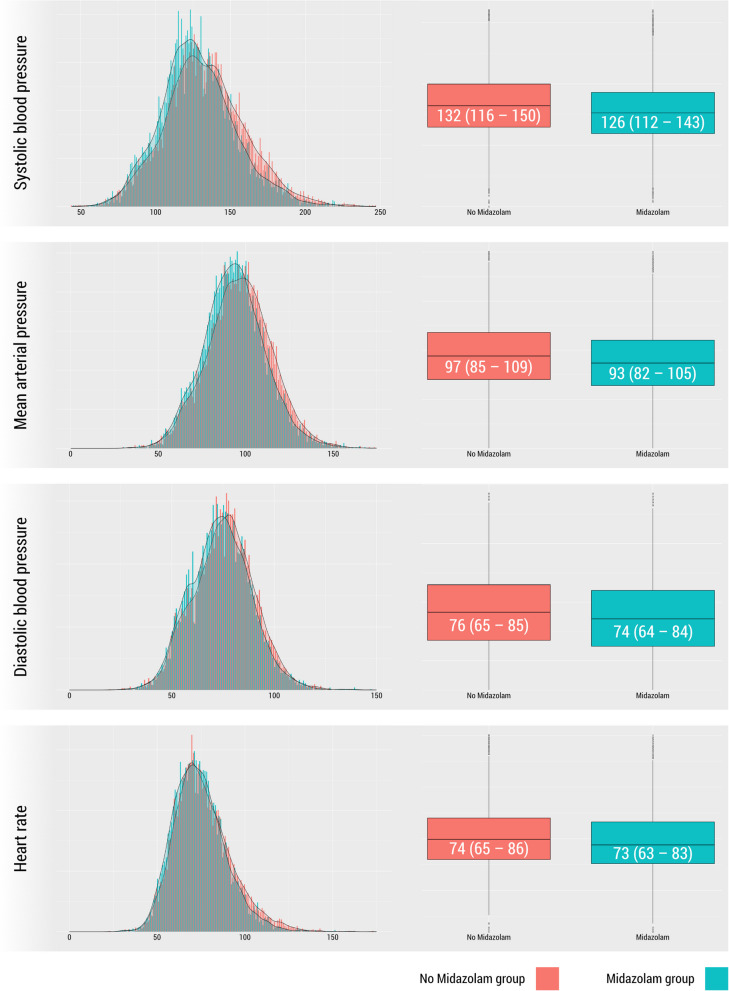
Results: After propensity score matching, we analyzed 7421 patients in each group. In this adjusted analysis, premedication with midazolam was not associated with mortality (OR 0.91, 95% CI 0.60 to 1.38, p = 0.662). Midazolam premedication was associated with significantly lower pre-induction blood pressures, with an estimated average treatment effect for systolic blood pressure of - 5.33 mmHg (SE 0.41, 95% CI - 6.13 to - 4.52 mmHg).
Conclusions: Midazolam prescription was not associated with increased mortality in a large cohort of surgical patients but with a lower pre-induction blood pressure and heart rate, suggesting a potential reduction in cardiovascular stress.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


