{"title":"结合血小板-淋巴细胞比值和脑脊液白细胞介素-8水平,辅助诊断格林-巴勒综合征和慢性炎性脱髓鞘性多神经病变。","authors":"Simin Song, Yunfei Bai, Haoran Mu, Jianru Xiao, Wei Li, Yuying Zhao, Chuanzhu Yan, Jinfan Zheng, Caijing Wang, Qinzhou Wang","doi":"10.1186/s12883-025-04330-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Guillain-Barré syndrome (GBS) and chronic inflammatory demyelinating polyneuropathy (CIDP) are immune-mediated neuropathies with overlapping clinical and electrophysiological features but distinct treatment strategies. This study investigated whether the platelet-to-lymphocyte ratio (PLR) and cerebrospinal fluid (CSF) interleukin-8 (IL-8) levels can serve as auxiliary biomarkers to aid in distinguishing CIDP from GBS.</p><p><strong>Methods: </strong>For 65 patients with GBS, 38 with typical CIDP, and 65 healthy controls (HCs), clinical, serological, and CSF data were collected. Inflammatory markers were analyzed. Binary logistic regression was performed to identify risk factors and establish a prediction model. Receiver operating characteristic (ROC) curves were used to assess diagnostic performance.</p><p><strong>Results: </strong>The neutrophil-to-lymphocyte ratio (NLR), derived NLR, PLR, Systemic Inflammation Response Index, and Systemic Immune-Inflammation Index levels were significantly higher in the GBS than in the CIDP or HC groups (P < 0.05). The lymphocyte count was significantly higher in patients with CIDP than in those with GBS (P < 0.01). CSF IgG and IL-8 (both P < 0.001) were significantly higher in patients with GBS than in those with CIDP. ROC curve analysis showed that the area under the curve (AUC) of PLR was 0.746 and that of CSF IL-8 was 0.786. Combining PLR and CSF IL-8 levels improved the AUC to 0.827 (95% CI: 0.749-0.905), with a specificity of 0.973.</p><p><strong>Conclusion: </strong>The combination of PLR and CSF IL-8 levels may serve as a useful adjunct to conventional clinical and electrophysiological assessments for differentiating CIDP from GBS. These findings also contribute to a better understanding of the immunological differences between acute and chronic inflammatory neuropathies.</p>","PeriodicalId":9170,"journal":{"name":"BMC Neurology","volume":"25 1","pages":"314"},"PeriodicalIF":2.2000,"publicationDate":"2025-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12312457/pdf/","citationCount":"0","resultStr":"{\"title\":\"An auxiliary diagnostic strategy for distinguishing Guillain-Barré syndrome and chronic inflammatory demyelinating polyneuropathy: combining platelet-to-lymphocyte ratio and cerebrospinal fluid interleukin-8 levels.\",\"authors\":\"Simin Song, Yunfei Bai, Haoran Mu, Jianru Xiao, Wei Li, Yuying Zhao, Chuanzhu Yan, Jinfan Zheng, Caijing Wang, Qinzhou Wang\",\"doi\":\"10.1186/s12883-025-04330-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Guillain-Barré syndrome (GBS) and chronic inflammatory demyelinating polyneuropathy (CIDP) are immune-mediated neuropathies with overlapping clinical and electrophysiological features but distinct treatment strategies. This study investigated whether the platelet-to-lymphocyte ratio (PLR) and cerebrospinal fluid (CSF) interleukin-8 (IL-8) levels can serve as auxiliary biomarkers to aid in distinguishing CIDP from GBS.</p><p><strong>Methods: </strong>For 65 patients with GBS, 38 with typical CIDP, and 65 healthy controls (HCs), clinical, serological, and CSF data were collected. Inflammatory markers were analyzed. Binary logistic regression was performed to identify risk factors and establish a prediction model. Receiver operating characteristic (ROC) curves were used to assess diagnostic performance.</p><p><strong>Results: </strong>The neutrophil-to-lymphocyte ratio (NLR), derived NLR, PLR, Systemic Inflammation Response Index, and Systemic Immune-Inflammation Index levels were significantly higher in the GBS than in the CIDP or HC groups (P < 0.05). The lymphocyte count was significantly higher in patients with CIDP than in those with GBS (P < 0.01). CSF IgG and IL-8 (both P < 0.001) were significantly higher in patients with GBS than in those with CIDP. ROC curve analysis showed that the area under the curve (AUC) of PLR was 0.746 and that of CSF IL-8 was 0.786. Combining PLR and CSF IL-8 levels improved the AUC to 0.827 (95% CI: 0.749-0.905), with a specificity of 0.973.</p><p><strong>Conclusion: </strong>The combination of PLR and CSF IL-8 levels may serve as a useful adjunct to conventional clinical and electrophysiological assessments for differentiating CIDP from GBS. These findings also contribute to a better understanding of the immunological differences between acute and chronic inflammatory neuropathies.</p>\",\"PeriodicalId\":9170,\"journal\":{\"name\":\"BMC Neurology\",\"volume\":\"25 1\",\"pages\":\"314\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-07-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12312457/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Neurology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12883-025-04330-1\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12883-025-04330-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
An auxiliary diagnostic strategy for distinguishing Guillain-Barré syndrome and chronic inflammatory demyelinating polyneuropathy: combining platelet-to-lymphocyte ratio and cerebrospinal fluid interleukin-8 levels.
Background: Guillain-Barré syndrome (GBS) and chronic inflammatory demyelinating polyneuropathy (CIDP) are immune-mediated neuropathies with overlapping clinical and electrophysiological features but distinct treatment strategies. This study investigated whether the platelet-to-lymphocyte ratio (PLR) and cerebrospinal fluid (CSF) interleukin-8 (IL-8) levels can serve as auxiliary biomarkers to aid in distinguishing CIDP from GBS.
Methods: For 65 patients with GBS, 38 with typical CIDP, and 65 healthy controls (HCs), clinical, serological, and CSF data were collected. Inflammatory markers were analyzed. Binary logistic regression was performed to identify risk factors and establish a prediction model. Receiver operating characteristic (ROC) curves were used to assess diagnostic performance.
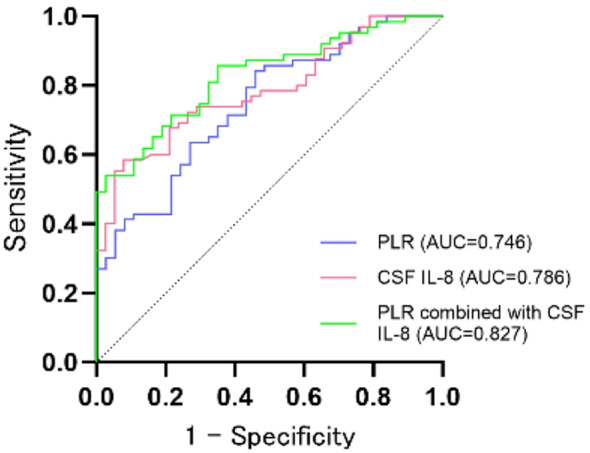
Results: The neutrophil-to-lymphocyte ratio (NLR), derived NLR, PLR, Systemic Inflammation Response Index, and Systemic Immune-Inflammation Index levels were significantly higher in the GBS than in the CIDP or HC groups (P < 0.05). The lymphocyte count was significantly higher in patients with CIDP than in those with GBS (P < 0.01). CSF IgG and IL-8 (both P < 0.001) were significantly higher in patients with GBS than in those with CIDP. ROC curve analysis showed that the area under the curve (AUC) of PLR was 0.746 and that of CSF IL-8 was 0.786. Combining PLR and CSF IL-8 levels improved the AUC to 0.827 (95% CI: 0.749-0.905), with a specificity of 0.973.
Conclusion: The combination of PLR and CSF IL-8 levels may serve as a useful adjunct to conventional clinical and electrophysiological assessments for differentiating CIDP from GBS. These findings also contribute to a better understanding of the immunological differences between acute and chronic inflammatory neuropathies.
期刊介绍:
BMC Neurology is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of neurological disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


