{"title":"肝硬化患者的难治性腹水","authors":"Madhumita Premkumar","doi":"10.1002/jgh3.70245","DOIUrl":null,"url":null,"abstract":"<p>Recurrent ascites refers to fluid accumulation in the abdomen that returns at least three times per year, despite dietary sodium restriction and diuretic treatment. It may precede the development of refractory ascites (RA). RA is characterized by ascites that cannot be resolved or whose early recurrence (after large volume paracentesis [LVP]) is not prevented by medical therapy [<span>1</span>]. RA is typically classified as either diuretic resistant or diuretic intolerant.</p><p>Management of RA includes ongoing sodium restriction with regular monitoring, frequent LVP, ≥ 5 L combined with infusion to prevent paracentesis-induced circulatory dysfunction, and possibly albumin infusions outside of paracentesis. For RA patients who do not respond to diuretics or experience significant side effects at maximum doses, alternative treatments should be considered, as further use increases complications without benefit. In the ANSWER study, Caraceni et al. [<span>2</span>] reported that long-term human albumin therapy improved overall survival in cirrhosis patients with uncomplicated ascites compared to standard treatment. Tolvaptan has been used as adjunctive therapy in patients with hyponatremia and RA [<span>3, 4</span>]. In suitable patients with preserved liver function, a covered, smaller-diameter transjugular-intrahepatic portosystemic shunt (TIPS) can improve quality of life and survival post-ascites clearance. Patients with RA are also likely to have recurrent episodes of hepatorenal syndrome-acute kidney injury (HRS-AKI) [<span>5</span>] and also cirrhotic cardiomyopathy (CCM) [<span>6</span>], which in turn impairs the health-related quality of life (HRQoL). For patients with RA who cannot undergo liver transplantation (LT) or TIPS, LVP and albumin infusion are the only treatments [<span>7</span>]. Future options may include automated low-flow ascites pumps [<span>8</span>].</p><p>LVPs are often needed weekly or fortnightly, straining hospital resources and causing unplanned admissions that reduce quality of life (QoL) and increase costs. Also, LVPs require point-of-care ultrasound guidance [<span>9</span>] to minimize the risks of bleeding [<span>10</span>] and infection.</p><p>Regular home drainage could prevent these frequent hospitalizations. As ascites drainage is palliative in patients unsuitable for LT, it should follow palliative care principles [<span>11</span>]. Indwelling catheters, commonly used in malignant ascites and hydrothorax, offer a viable care model.</p><p>In this issue of JGHOpen, Ramachandran et al. [<span>12</span>] describe the palliative impact of long-term abdominal drain (LTAD) insertion in patients with RA. Fifty-one cirrhosis patients with RA were screened; 7 underwent LT, 6 chose TIPS, and 12 had drains inserted for analysis. Six deaths occurred; none related to LTAD. All participants preferred LTAD over LVPs and were highly satisfied. Of the four who completed 6 months, three continued LTAD; the fourth had improved liver function after abstaining from alcohol. Drains carry a significant risk of complications—two cases of spontaneous bacterial peritonitis occurred: one due to missed antibiotics, the other from repeated drain adjustments. Both infections resolved with IV antibiotics without removing the LTAD. Local complications, including cellulitis and leakage, were mild and non-serious.</p><p>Patients with RA should be evaluated for liver transplantation (LT) given the associated poor prognosis. In a randomized controlled trial conducted by Macken et al. [<span>13</span>], 36 patients were assigned to either long-term abdominal drain (<i>n</i> = 17) or large-volume paracentesis (LVPs, <i>n</i> = 19). The incidence of self-limiting cellulitis or leakage was 41% (7/17) in the long-term abdominal drain group compared to 11% (2/19) in the LVP group. Peritonitis occurred in 6% (1/17) of patients in the long-term drain group versus 11% (2/19) in the LVP group. Again, it is unclear if long-term albumin therapy should be used in patients with LTAD [<span>14</span>].</p><p>Key unresolved issues include optimal long-term albumin use, beta-blocker application, ideal TIPS timing, and best stent diameter for minimizing shunt-related side effects in ascites management [<span>15</span>]. Lastly, patients often receive SBP prophylaxis with mixed results. In the current study, prescribing antibiotics as primary prophylaxis to all trial participants to prevent SBP is also not supported based on updated evidence [<span>16</span>]. Long-term use of antibiotics presents risks to individuals and the wider population, increasing antimicrobial resistance, so future trials should thoughtfully consider this strategy [<span>17</span>]. The management of ascites should therefore be personalized to suit the goals of care for a patient [<span>18</span>]. Other medications that have been used in small studies include the use of midodrine for elevating the mean arterial pressure and improving diuretic response [<span>19</span>] and the use of Sodium glucose cotransporters to improve diuresis by augmenting glycosuria. Patients with CCM and diastolic heart failure may benefit from the addition of drugs like empagliflozin, which has been shown to improve control of ascites in small studies and has ameliorated cardiac dysfunction through pleiotropic effects [<span>20</span>]. Figure 1 shows the current need for personalized management of patients with RA. The best result will be to perform a liver transplantation, but it may not be feasible in resource-constrained settings.</p><p>While LTAD provides clear benefits for patients and carers, it raises broader questions about the factors influencing HRQoL in end-stage liver disease. LTADs are only one part of the solution; addressing the wider challenges faced by these individuals remains an ongoing issue. Therefore, the current study adds to resolving the clinical conundrum faced by clinicians who care for patients with RA, who are not eligible for LT or TIPS. It may offer a marginal benefit over frequent LVP in a small subset of individuals.</p><p>M.P. serves as an associate editor of JGHOpen and was blinded to the peer review and editorial decision of this manuscript. The author declares no conflicts of interest.</p>","PeriodicalId":45861,"journal":{"name":"JGH Open","volume":"9 8","pages":""},"PeriodicalIF":1.5000,"publicationDate":"2025-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jgh3.70245","citationCount":"0","resultStr":"{\"title\":\"Refractory Ascites in Patients With Cirrhosis\",\"authors\":\"Madhumita Premkumar\",\"doi\":\"10.1002/jgh3.70245\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Recurrent ascites refers to fluid accumulation in the abdomen that returns at least three times per year, despite dietary sodium restriction and diuretic treatment. It may precede the development of refractory ascites (RA). RA is characterized by ascites that cannot be resolved or whose early recurrence (after large volume paracentesis [LVP]) is not prevented by medical therapy [<span>1</span>]. RA is typically classified as either diuretic resistant or diuretic intolerant.</p><p>Management of RA includes ongoing sodium restriction with regular monitoring, frequent LVP, ≥ 5 L combined with infusion to prevent paracentesis-induced circulatory dysfunction, and possibly albumin infusions outside of paracentesis. For RA patients who do not respond to diuretics or experience significant side effects at maximum doses, alternative treatments should be considered, as further use increases complications without benefit. In the ANSWER study, Caraceni et al. [<span>2</span>] reported that long-term human albumin therapy improved overall survival in cirrhosis patients with uncomplicated ascites compared to standard treatment. Tolvaptan has been used as adjunctive therapy in patients with hyponatremia and RA [<span>3, 4</span>]. In suitable patients with preserved liver function, a covered, smaller-diameter transjugular-intrahepatic portosystemic shunt (TIPS) can improve quality of life and survival post-ascites clearance. Patients with RA are also likely to have recurrent episodes of hepatorenal syndrome-acute kidney injury (HRS-AKI) [<span>5</span>] and also cirrhotic cardiomyopathy (CCM) [<span>6</span>], which in turn impairs the health-related quality of life (HRQoL). For patients with RA who cannot undergo liver transplantation (LT) or TIPS, LVP and albumin infusion are the only treatments [<span>7</span>]. Future options may include automated low-flow ascites pumps [<span>8</span>].</p><p>LVPs are often needed weekly or fortnightly, straining hospital resources and causing unplanned admissions that reduce quality of life (QoL) and increase costs. Also, LVPs require point-of-care ultrasound guidance [<span>9</span>] to minimize the risks of bleeding [<span>10</span>] and infection.</p><p>Regular home drainage could prevent these frequent hospitalizations. As ascites drainage is palliative in patients unsuitable for LT, it should follow palliative care principles [<span>11</span>]. Indwelling catheters, commonly used in malignant ascites and hydrothorax, offer a viable care model.</p><p>In this issue of JGHOpen, Ramachandran et al. [<span>12</span>] describe the palliative impact of long-term abdominal drain (LTAD) insertion in patients with RA. Fifty-one cirrhosis patients with RA were screened; 7 underwent LT, 6 chose TIPS, and 12 had drains inserted for analysis. Six deaths occurred; none related to LTAD. All participants preferred LTAD over LVPs and were highly satisfied. Of the four who completed 6 months, three continued LTAD; the fourth had improved liver function after abstaining from alcohol. Drains carry a significant risk of complications—two cases of spontaneous bacterial peritonitis occurred: one due to missed antibiotics, the other from repeated drain adjustments. Both infections resolved with IV antibiotics without removing the LTAD. Local complications, including cellulitis and leakage, were mild and non-serious.</p><p>Patients with RA should be evaluated for liver transplantation (LT) given the associated poor prognosis. In a randomized controlled trial conducted by Macken et al. [<span>13</span>], 36 patients were assigned to either long-term abdominal drain (<i>n</i> = 17) or large-volume paracentesis (LVPs, <i>n</i> = 19). The incidence of self-limiting cellulitis or leakage was 41% (7/17) in the long-term abdominal drain group compared to 11% (2/19) in the LVP group. Peritonitis occurred in 6% (1/17) of patients in the long-term drain group versus 11% (2/19) in the LVP group. Again, it is unclear if long-term albumin therapy should be used in patients with LTAD [<span>14</span>].</p><p>Key unresolved issues include optimal long-term albumin use, beta-blocker application, ideal TIPS timing, and best stent diameter for minimizing shunt-related side effects in ascites management [<span>15</span>]. Lastly, patients often receive SBP prophylaxis with mixed results. In the current study, prescribing antibiotics as primary prophylaxis to all trial participants to prevent SBP is also not supported based on updated evidence [<span>16</span>]. Long-term use of antibiotics presents risks to individuals and the wider population, increasing antimicrobial resistance, so future trials should thoughtfully consider this strategy [<span>17</span>]. The management of ascites should therefore be personalized to suit the goals of care for a patient [<span>18</span>]. Other medications that have been used in small studies include the use of midodrine for elevating the mean arterial pressure and improving diuretic response [<span>19</span>] and the use of Sodium glucose cotransporters to improve diuresis by augmenting glycosuria. Patients with CCM and diastolic heart failure may benefit from the addition of drugs like empagliflozin, which has been shown to improve control of ascites in small studies and has ameliorated cardiac dysfunction through pleiotropic effects [<span>20</span>]. Figure 1 shows the current need for personalized management of patients with RA. The best result will be to perform a liver transplantation, but it may not be feasible in resource-constrained settings.</p><p>While LTAD provides clear benefits for patients and carers, it raises broader questions about the factors influencing HRQoL in end-stage liver disease. LTADs are only one part of the solution; addressing the wider challenges faced by these individuals remains an ongoing issue. Therefore, the current study adds to resolving the clinical conundrum faced by clinicians who care for patients with RA, who are not eligible for LT or TIPS. It may offer a marginal benefit over frequent LVP in a small subset of individuals.</p><p>M.P. serves as an associate editor of JGHOpen and was blinded to the peer review and editorial decision of this manuscript. The author declares no conflicts of interest.</p>\",\"PeriodicalId\":45861,\"journal\":{\"name\":\"JGH Open\",\"volume\":\"9 8\",\"pages\":\"\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-07-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jgh3.70245\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JGH Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.70245\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JGH Open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.70245","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
复发性腹水是指腹腔积液,每年至少复发三次,尽管饮食限制钠和利尿剂治疗。它可能先于难治性腹水(RA)的发展。RA的特点是腹水无法解决或早期复发(在大容量穿刺[LVP]后)无法通过药物治疗预防[10]。类风湿性关节炎通常分为利尿剂耐药和利尿剂不耐受。RA的治疗包括持续限制钠并定期监测,频繁的LVP,≥5l联合输注以防止穿刺诱导的循环功能障碍,并可能在穿刺外输注白蛋白。对于对利尿剂无反应或在最大剂量下出现明显副作用的RA患者,应考虑替代治疗,因为进一步使用利尿剂会增加并发症而无益处。在ANSWER研究中,Caraceni等人报道,与标准治疗相比,长期人白蛋白治疗可提高肝硬化合并无并发症腹水患者的总生存率。托伐普坦已被用作低钠血症和RA患者的辅助治疗[3,4]。在肝功能保留的合适患者中,一个覆盖的,较小直径的经颈静脉-肝内门体分流术(TIPS)可以改善生活质量和腹水清除后的生存率。RA患者也可能反复发作肝肾综合征-急性肾损伤(HRS-AKI)[5]和肝硬化心肌病(CCM)[6],这反过来又损害了健康相关的生活质量(HRQoL)。对于不能接受肝移植(LT)或TIPS的RA患者,LVP和白蛋白输注是唯一的治疗方法。未来的选择可能包括自动低流量腹水泵[8]。lvp通常需要每周或每两周进行一次,这使医院资源紧张,并导致意外入院,从而降低了生活质量(QoL)并增加了成本。此外,LVPs需要即时超声引导,以尽量减少出血和感染的风险。定期的家庭引流可以防止这些频繁的住院治疗。由于腹水引流对不适合肝移植的患者是姑息性的,因此应遵循姑息治疗原则[11]。留置导尿管常用于恶性腹水和胸腔积液,提供了一种可行的护理模式。在本期JGHOpen中,Ramachandran等人描述了长期腹腔引流管(LTAD)插入对RA患者的缓解作用。筛查51例肝硬化类风湿性关节炎患者;7例行肝移植,6例行TIPS, 12例置入引流管进行分析。6人死亡;与LTAD无关。所有参与者都更喜欢LTAD而不是lvp,并且非常满意。完成6个月治疗的4人中,有3人继续LTAD治疗;第四名患者在戒酒后肝功能有所改善。引流管有很大的并发症风险——发生了两例自发性细菌性腹膜炎:一例是由于漏用抗生素,另一例是由于反复调整引流管。两种感染均通过静脉注射抗生素解决,无需移除LTAD。局部并发症,包括蜂窝织炎和渗漏,轻微和不严重。考虑到相关的不良预后,RA患者应评估肝移植(LT)。在Macken等人进行的一项随机对照试验中,36例患者被分配到长期腹腔引流(n = 17)或大容量穿刺(LVPs, n = 19)。长期腹腔引流组的自限性蜂窝织炎或渗漏发生率为41%(7/17),而LVP组为11%(2/19)。长期引流组有6%(1/17)的患者发生腹膜炎,而LVP组有11%(2/19)的患者发生腹膜炎。同样,长期白蛋白治疗是否应该用于LTAD患者尚不清楚。关键的未解决的问题包括最佳的长期白蛋白使用,β受体阻滞剂的应用,理想的TIPS时机,以及在腹水管理中最小化分流相关副作用的最佳支架直径[15]。最后,患者经常接受收缩压预防,结果好坏参半。在目前的研究中,根据最新的证据[16],也不支持将抗生素作为所有试验参与者预防收缩压的初级预防措施。长期使用抗生素会给个人和更广泛的人群带来风险,增加抗菌素耐药性,因此未来的试验应仔细考虑这一策略。因此,腹水的处理应个性化,以适应患者的护理目标。在小型研究中使用的其他药物包括使用midodrine来提高平均动脉压和改善利尿反应b[19],以及使用葡萄糖共转运体钠通过增加糖尿来改善利尿。 CCM和舒张性心力衰竭的患者可能受益于加入恩格列净等药物,在小型研究中已被证明可以改善腹水的控制,并通过多效性作用改善心功能障碍。图1显示了目前对RA患者个性化管理的需求。最好的结果是进行肝移植,但在资源有限的情况下可能不可行。虽然LTAD为患者和护理人员提供了明显的好处,但它提出了影响终末期肝病患者HRQoL的因素的更广泛的问题。ltad只是解决方案的一部分;解决这些人面临的更广泛的挑战仍然是一个持续的问题。因此,目前的研究增加了解决临床医生所面临的临床难题,这些临床医生照顾RA患者,他们不符合LT或TIPS的条件。在一小部分个体中,它可能比频繁的LVP提供边际效益。作为JGHOpen的副主编,对该稿件的同行评议和编辑决定不知情。作者声明无利益冲突。
Recurrent ascites refers to fluid accumulation in the abdomen that returns at least three times per year, despite dietary sodium restriction and diuretic treatment. It may precede the development of refractory ascites (RA). RA is characterized by ascites that cannot be resolved or whose early recurrence (after large volume paracentesis [LVP]) is not prevented by medical therapy [1]. RA is typically classified as either diuretic resistant or diuretic intolerant.
Management of RA includes ongoing sodium restriction with regular monitoring, frequent LVP, ≥ 5 L combined with infusion to prevent paracentesis-induced circulatory dysfunction, and possibly albumin infusions outside of paracentesis. For RA patients who do not respond to diuretics or experience significant side effects at maximum doses, alternative treatments should be considered, as further use increases complications without benefit. In the ANSWER study, Caraceni et al. [2] reported that long-term human albumin therapy improved overall survival in cirrhosis patients with uncomplicated ascites compared to standard treatment. Tolvaptan has been used as adjunctive therapy in patients with hyponatremia and RA [3, 4]. In suitable patients with preserved liver function, a covered, smaller-diameter transjugular-intrahepatic portosystemic shunt (TIPS) can improve quality of life and survival post-ascites clearance. Patients with RA are also likely to have recurrent episodes of hepatorenal syndrome-acute kidney injury (HRS-AKI) [5] and also cirrhotic cardiomyopathy (CCM) [6], which in turn impairs the health-related quality of life (HRQoL). For patients with RA who cannot undergo liver transplantation (LT) or TIPS, LVP and albumin infusion are the only treatments [7]. Future options may include automated low-flow ascites pumps [8].
LVPs are often needed weekly or fortnightly, straining hospital resources and causing unplanned admissions that reduce quality of life (QoL) and increase costs. Also, LVPs require point-of-care ultrasound guidance [9] to minimize the risks of bleeding [10] and infection.
Regular home drainage could prevent these frequent hospitalizations. As ascites drainage is palliative in patients unsuitable for LT, it should follow palliative care principles [11]. Indwelling catheters, commonly used in malignant ascites and hydrothorax, offer a viable care model.
In this issue of JGHOpen, Ramachandran et al. [12] describe the palliative impact of long-term abdominal drain (LTAD) insertion in patients with RA. Fifty-one cirrhosis patients with RA were screened; 7 underwent LT, 6 chose TIPS, and 12 had drains inserted for analysis. Six deaths occurred; none related to LTAD. All participants preferred LTAD over LVPs and were highly satisfied. Of the four who completed 6 months, three continued LTAD; the fourth had improved liver function after abstaining from alcohol. Drains carry a significant risk of complications—two cases of spontaneous bacterial peritonitis occurred: one due to missed antibiotics, the other from repeated drain adjustments. Both infections resolved with IV antibiotics without removing the LTAD. Local complications, including cellulitis and leakage, were mild and non-serious.
Patients with RA should be evaluated for liver transplantation (LT) given the associated poor prognosis. In a randomized controlled trial conducted by Macken et al. [13], 36 patients were assigned to either long-term abdominal drain (n = 17) or large-volume paracentesis (LVPs, n = 19). The incidence of self-limiting cellulitis or leakage was 41% (7/17) in the long-term abdominal drain group compared to 11% (2/19) in the LVP group. Peritonitis occurred in 6% (1/17) of patients in the long-term drain group versus 11% (2/19) in the LVP group. Again, it is unclear if long-term albumin therapy should be used in patients with LTAD [14].
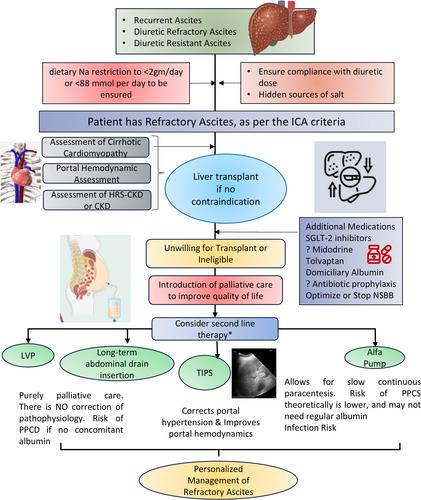
Key unresolved issues include optimal long-term albumin use, beta-blocker application, ideal TIPS timing, and best stent diameter for minimizing shunt-related side effects in ascites management [15]. Lastly, patients often receive SBP prophylaxis with mixed results. In the current study, prescribing antibiotics as primary prophylaxis to all trial participants to prevent SBP is also not supported based on updated evidence [16]. Long-term use of antibiotics presents risks to individuals and the wider population, increasing antimicrobial resistance, so future trials should thoughtfully consider this strategy [17]. The management of ascites should therefore be personalized to suit the goals of care for a patient [18]. Other medications that have been used in small studies include the use of midodrine for elevating the mean arterial pressure and improving diuretic response [19] and the use of Sodium glucose cotransporters to improve diuresis by augmenting glycosuria. Patients with CCM and diastolic heart failure may benefit from the addition of drugs like empagliflozin, which has been shown to improve control of ascites in small studies and has ameliorated cardiac dysfunction through pleiotropic effects [20]. Figure 1 shows the current need for personalized management of patients with RA. The best result will be to perform a liver transplantation, but it may not be feasible in resource-constrained settings.
While LTAD provides clear benefits for patients and carers, it raises broader questions about the factors influencing HRQoL in end-stage liver disease. LTADs are only one part of the solution; addressing the wider challenges faced by these individuals remains an ongoing issue. Therefore, the current study adds to resolving the clinical conundrum faced by clinicians who care for patients with RA, who are not eligible for LT or TIPS. It may offer a marginal benefit over frequent LVP in a small subset of individuals.
M.P. serves as an associate editor of JGHOpen and was blinded to the peer review and editorial decision of this manuscript. The author declares no conflicts of interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


