Gabrielle Brown, Pavlos Msaouel, Avital M. Miller, Ramez Kouzy, Timothy A. Lin, Joseph Abi Jaoude, Ethan B. Ludmir, Alexander D. Sherry
{"title":"肿瘤学III期随机试验中的患者、医生和评估员盲法:一项荟萃流行病学分析","authors":"Gabrielle Brown, Pavlos Msaouel, Avital M. Miller, Ramez Kouzy, Timothy A. Lin, Joseph Abi Jaoude, Ethan B. Ludmir, Alexander D. Sherry","doi":"10.1002/cam4.71097","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Blinding mitigates bias in randomized trials and may be especially crucial for surrogate endpoints, such as progression-free survival (PFS). Here, we characterize utilization of and factors associated with blinding in Phase III oncology trials with PFS primary endpoints.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Two-arm, superiority-design trials investigating systemic therapy were identified in May 2024 from ClinicalTrials.gov with no date limitation. Trials were required to have a PFS primary endpoint. The study outcomes were the presence of double-blind designs and blinded independent central review (BICR) for the primary endpoint. Ninety-five percent credible intervals for binary outcomes were estimated from beta distributions, and multivariable logistic regressions explored associations with trial-level features.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>After screening, 237 trials were included, enrolling 127,518 patients. A double-blind design was used in 105 trials (44%, 95% CrI 38%–51%). BICR was used in 111 trials (47%, 95% CrI 41%–53%), including 39 double-blind trials (16%, 95% CrI 12%–22%). Trials with BICR had higher odds of meeting the primary endpoint (OR 1.84; 95% CI 1.06–3.18; <i>p</i> = 0.03). The PFS assessor identity (central vs. local) or blinding status was not reported in 50 trials (26%, 95% CrI 16%–27%). Trials that met prespecified significance criteria for PFS were more likely to report whether PFS assessors were blinded/unblinded and central/local (OR, 3.05; 95% Cl: 1.60–5.81; <i>p</i> = 0.0007).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Despite the importance of double blinding in combination with BICR for reducing bias, only a few trials blinded physicians, patients, and primary endpoint assessors. This meta-epidemiological study illuminates the prevalence of potential assessment biases affecting PFS in Phase III oncology and secondarily emphasizes the need for improved methodology reporting.</p>\n </section>\n </div>","PeriodicalId":139,"journal":{"name":"Cancer Medicine","volume":"14 15","pages":""},"PeriodicalIF":3.1000,"publicationDate":"2025-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cam4.71097","citationCount":"0","resultStr":"{\"title\":\"Patient, Physician, and Assessor Blinding in Phase III Randomized Trials in Oncology: A Meta-Epidemiological Analysis\",\"authors\":\"Gabrielle Brown, Pavlos Msaouel, Avital M. Miller, Ramez Kouzy, Timothy A. Lin, Joseph Abi Jaoude, Ethan B. Ludmir, Alexander D. Sherry\",\"doi\":\"10.1002/cam4.71097\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Blinding mitigates bias in randomized trials and may be especially crucial for surrogate endpoints, such as progression-free survival (PFS). Here, we characterize utilization of and factors associated with blinding in Phase III oncology trials with PFS primary endpoints.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Two-arm, superiority-design trials investigating systemic therapy were identified in May 2024 from ClinicalTrials.gov with no date limitation. Trials were required to have a PFS primary endpoint. The study outcomes were the presence of double-blind designs and blinded independent central review (BICR) for the primary endpoint. Ninety-five percent credible intervals for binary outcomes were estimated from beta distributions, and multivariable logistic regressions explored associations with trial-level features.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>After screening, 237 trials were included, enrolling 127,518 patients. A double-blind design was used in 105 trials (44%, 95% CrI 38%–51%). BICR was used in 111 trials (47%, 95% CrI 41%–53%), including 39 double-blind trials (16%, 95% CrI 12%–22%). Trials with BICR had higher odds of meeting the primary endpoint (OR 1.84; 95% CI 1.06–3.18; <i>p</i> = 0.03). The PFS assessor identity (central vs. local) or blinding status was not reported in 50 trials (26%, 95% CrI 16%–27%). Trials that met prespecified significance criteria for PFS were more likely to report whether PFS assessors were blinded/unblinded and central/local (OR, 3.05; 95% Cl: 1.60–5.81; <i>p</i> = 0.0007).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Despite the importance of double blinding in combination with BICR for reducing bias, only a few trials blinded physicians, patients, and primary endpoint assessors. This meta-epidemiological study illuminates the prevalence of potential assessment biases affecting PFS in Phase III oncology and secondarily emphasizes the need for improved methodology reporting.</p>\\n </section>\\n </div>\",\"PeriodicalId\":139,\"journal\":{\"name\":\"Cancer Medicine\",\"volume\":\"14 15\",\"pages\":\"\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-07-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cam4.71097\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cam4.71097\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cam4.71097","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Patient, Physician, and Assessor Blinding in Phase III Randomized Trials in Oncology: A Meta-Epidemiological Analysis
Background
Blinding mitigates bias in randomized trials and may be especially crucial for surrogate endpoints, such as progression-free survival (PFS). Here, we characterize utilization of and factors associated with blinding in Phase III oncology trials with PFS primary endpoints.
Methods
Two-arm, superiority-design trials investigating systemic therapy were identified in May 2024 from ClinicalTrials.gov with no date limitation. Trials were required to have a PFS primary endpoint. The study outcomes were the presence of double-blind designs and blinded independent central review (BICR) for the primary endpoint. Ninety-five percent credible intervals for binary outcomes were estimated from beta distributions, and multivariable logistic regressions explored associations with trial-level features.
Results
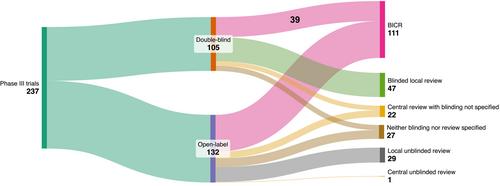
After screening, 237 trials were included, enrolling 127,518 patients. A double-blind design was used in 105 trials (44%, 95% CrI 38%–51%). BICR was used in 111 trials (47%, 95% CrI 41%–53%), including 39 double-blind trials (16%, 95% CrI 12%–22%). Trials with BICR had higher odds of meeting the primary endpoint (OR 1.84; 95% CI 1.06–3.18; p = 0.03). The PFS assessor identity (central vs. local) or blinding status was not reported in 50 trials (26%, 95% CrI 16%–27%). Trials that met prespecified significance criteria for PFS were more likely to report whether PFS assessors were blinded/unblinded and central/local (OR, 3.05; 95% Cl: 1.60–5.81; p = 0.0007).
Conclusions
Despite the importance of double blinding in combination with BICR for reducing bias, only a few trials blinded physicians, patients, and primary endpoint assessors. This meta-epidemiological study illuminates the prevalence of potential assessment biases affecting PFS in Phase III oncology and secondarily emphasizes the need for improved methodology reporting.
期刊介绍:
Cancer Medicine is a peer-reviewed, open access, interdisciplinary journal providing rapid publication of research from global biomedical researchers across the cancer sciences. The journal will consider submissions from all oncologic specialties, including, but not limited to, the following areas:
Clinical Cancer Research
Translational research ∙ clinical trials ∙ chemotherapy ∙ radiation therapy ∙ surgical therapy ∙ clinical observations ∙ clinical guidelines ∙ genetic consultation ∙ ethical considerations
Cancer Biology:
Molecular biology ∙ cellular biology ∙ molecular genetics ∙ genomics ∙ immunology ∙ epigenetics ∙ metabolic studies ∙ proteomics ∙ cytopathology ∙ carcinogenesis ∙ drug discovery and delivery.
Cancer Prevention:
Behavioral science ∙ psychosocial studies ∙ screening ∙ nutrition ∙ epidemiology and prevention ∙ community outreach.
Bioinformatics:
Gene expressions profiles ∙ gene regulation networks ∙ genome bioinformatics ∙ pathwayanalysis ∙ prognostic biomarkers.
Cancer Medicine publishes original research articles, systematic reviews, meta-analyses, and research methods papers, along with invited editorials and commentaries. Original research papers must report well-conducted research with conclusions supported by the data presented in the paper.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


