Qianyu Shi, Jiazhi Zhu, Haijie Liang, Ruifeng Wang, Siyi Huang, Wei Guo, Tao Ji, Xiaodong Tang
{"title":"使用3D打印技术进行全骶骨切除术和重建的准确性:连续9例的准确性验证。","authors":"Qianyu Shi, Jiazhi Zhu, Haijie Liang, Ruifeng Wang, Siyi Huang, Wei Guo, Tao Ji, Xiaodong Tang","doi":"10.1186/s41205-025-00295-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>With 3D printing technology, we can now use preoperative imaging for precise surgical plan. We can also use patient-specific surgical jig to improve the accuracy of osteotomy and 3D-printed custom-made endoprostheses combined with a screw-rod system to restore lumbosacral stability. The aim of this study was to evaluate the accuracy of 3D printing technology for precise osteotomy during total sacrectomy.</p><p><strong>Methods: </strong>Nine patients with primary malignant tumors of the sacrum who underwent total sacrectomy at our center were enrolled. Osteotomy was planned based on preoperative imaging (CT, MRI). Generally, an additional 8-10 mm margin beyond the tumor was determined by the fusion of MR and CT images. Patient-specific surgical jigs and 3D-printed sacral endoprostheses were then designed based on the planned osteotomy planes. Pre- and postoperative 3D models of the lumbosacral and pelvic regions were constructed using the fiducial registration model of 3D slicer software 5.1.0. Postoperative CT scans were compared with the planned osteomy planes based on preoperative CT scans, in order to evaluate the accuracy of the osteotomy and endoprosthetic reconstruction. For each patient, four levels of osteotomy planes were chosen, including the upper edge of the sacroiliac (SI) joint, the S1 and S2 foramen levels, and the caudal edge of the SI joint, for analyzing position and angular deviations between the preoperative plan and actual osteotomy along with the endoprosthesis position.</p><p><strong>Results: </strong>Pathological diagnoses included four cases of osteosarcoma, four cases of chordoma, and one case of Ewing sarcoma. All osteotomies in nine patients achieved R0 resection, as verified pathologically. An average angular deviation of 4.27° (interquartile range[IQR] 4.15) and an osteotomy position deviation of 4.00 mm (IQR 2.90) were observed. The mean angular deviations of the four levels were 3.50° (IQR 6.02), 3.86° (IQR 2.55), 4.81° (IQR 4.37), and 4.92° (IQR 3.27). The mean position deviations at the four levels were 3.15 mm (IQR 3.54), 3.55 mm (IQR 1.37), 4.26 mm (IQR 2.61), and 4.86 mm (IQR 3.93). No significant difference was found among the angular and position deviations at different levels. However, the proportions of individuals with position deviations > 2 mm and > 5 mm were significantly greater at the caudal end of the SI joint than at the upper end. All position deviations were within 8 mm. The average follow-up duration was 24.4 months. At the last follow-up, three patients experienced local recurrence, and one patient died of disease. All endoprostheses were in place without significant displacement. The mean Musculoskeletal Tumor Society scoring system (MSTS93) and MUD scores (function and sensation of lower limbs (M), urination and uriesthesia (U), and defecation and rectal sensation (D)) were 19.4 (16 to 24) and 16.3 (12 to 24), respectively.</p><p><strong>Conclusion: </strong>Notably, 3D-printed patient-specific surgical jigs exhibit high accuracy of osteotomy and lead to optimal surgical margin and reconstruction in total sacrectomy. Effective and reliable reconstruction can be achieved with a custom-made 3D-printed endoprosthesis. The application of 3D printing technology using patient-specific surgical jigs and the custom-made 3D-printed implants exhibited high surgical accuracy in total sacrectomy, as evidenced by accuracy validation.</p>","PeriodicalId":72036,"journal":{"name":"3D printing in medicine","volume":"11 1","pages":"42"},"PeriodicalIF":3.1000,"publicationDate":"2025-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12308921/pdf/","citationCount":"0","resultStr":"{\"title\":\"How precise is excision and reconstruction using 3D printing technology for total sacrectomy: accuracy validation in 9 consecutive cases.\",\"authors\":\"Qianyu Shi, Jiazhi Zhu, Haijie Liang, Ruifeng Wang, Siyi Huang, Wei Guo, Tao Ji, Xiaodong Tang\",\"doi\":\"10.1186/s41205-025-00295-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>With 3D printing technology, we can now use preoperative imaging for precise surgical plan. We can also use patient-specific surgical jig to improve the accuracy of osteotomy and 3D-printed custom-made endoprostheses combined with a screw-rod system to restore lumbosacral stability. The aim of this study was to evaluate the accuracy of 3D printing technology for precise osteotomy during total sacrectomy.</p><p><strong>Methods: </strong>Nine patients with primary malignant tumors of the sacrum who underwent total sacrectomy at our center were enrolled. Osteotomy was planned based on preoperative imaging (CT, MRI). Generally, an additional 8-10 mm margin beyond the tumor was determined by the fusion of MR and CT images. Patient-specific surgical jigs and 3D-printed sacral endoprostheses were then designed based on the planned osteotomy planes. Pre- and postoperative 3D models of the lumbosacral and pelvic regions were constructed using the fiducial registration model of 3D slicer software 5.1.0. Postoperative CT scans were compared with the planned osteomy planes based on preoperative CT scans, in order to evaluate the accuracy of the osteotomy and endoprosthetic reconstruction. For each patient, four levels of osteotomy planes were chosen, including the upper edge of the sacroiliac (SI) joint, the S1 and S2 foramen levels, and the caudal edge of the SI joint, for analyzing position and angular deviations between the preoperative plan and actual osteotomy along with the endoprosthesis position.</p><p><strong>Results: </strong>Pathological diagnoses included four cases of osteosarcoma, four cases of chordoma, and one case of Ewing sarcoma. All osteotomies in nine patients achieved R0 resection, as verified pathologically. An average angular deviation of 4.27° (interquartile range[IQR] 4.15) and an osteotomy position deviation of 4.00 mm (IQR 2.90) were observed. The mean angular deviations of the four levels were 3.50° (IQR 6.02), 3.86° (IQR 2.55), 4.81° (IQR 4.37), and 4.92° (IQR 3.27). The mean position deviations at the four levels were 3.15 mm (IQR 3.54), 3.55 mm (IQR 1.37), 4.26 mm (IQR 2.61), and 4.86 mm (IQR 3.93). No significant difference was found among the angular and position deviations at different levels. However, the proportions of individuals with position deviations > 2 mm and > 5 mm were significantly greater at the caudal end of the SI joint than at the upper end. All position deviations were within 8 mm. The average follow-up duration was 24.4 months. At the last follow-up, three patients experienced local recurrence, and one patient died of disease. All endoprostheses were in place without significant displacement. The mean Musculoskeletal Tumor Society scoring system (MSTS93) and MUD scores (function and sensation of lower limbs (M), urination and uriesthesia (U), and defecation and rectal sensation (D)) were 19.4 (16 to 24) and 16.3 (12 to 24), respectively.</p><p><strong>Conclusion: </strong>Notably, 3D-printed patient-specific surgical jigs exhibit high accuracy of osteotomy and lead to optimal surgical margin and reconstruction in total sacrectomy. Effective and reliable reconstruction can be achieved with a custom-made 3D-printed endoprosthesis. The application of 3D printing technology using patient-specific surgical jigs and the custom-made 3D-printed implants exhibited high surgical accuracy in total sacrectomy, as evidenced by accuracy validation.</p>\",\"PeriodicalId\":72036,\"journal\":{\"name\":\"3D printing in medicine\",\"volume\":\"11 1\",\"pages\":\"42\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-07-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12308921/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"3D printing in medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41205-025-00295-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"3D printing in medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41205-025-00295-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
摘要
背景:随着3D打印技术的发展,我们现在可以利用术前成像来制定精确的手术计划。我们还可以使用患者特定的手术夹具来提高截骨的准确性,并使用3d打印定制的内假体结合螺钉杆系统来恢复腰骶稳定性。本研究的目的是评估3D打印技术在全骶骨切除术中精确截骨的准确性。方法:9例骶骨原发恶性肿瘤患者在我院行全骶骨切除术。根据术前影像学(CT、MRI)计划截骨。通常,通过MR和CT图像的融合来确定肿瘤外的额外8- 10mm边缘。然后根据计划的截骨平面设计患者特定的手术夹具和3d打印的骶骨内假体。采用三维切片机软件5.1.0的基准配准模型,建立腰骶、骨盆区域术前、术后三维模型。将术后CT扫描与术前CT扫描计划的截骨平面进行比较,以评估截骨和假体内重建的准确性。每位患者选择4个截骨平面,包括骶髂关节上缘、骶髂关节S1、骶髂关节S2孔水平和骶髂关节尾侧边缘,分析术前计划与实际截骨以及假体位置之间的位置和角度偏差。结果:病理诊断为骨原性肉瘤4例,脊索瘤4例,尤文氏肉瘤1例。经病理证实,9例患者的截骨术均达到R0切除。平均角度偏差为4.27°(四分位间距[IQR] 4.15),截骨位置偏差为4.00 mm (IQR 2.90)。四个水平的平均角度偏差分别为3.50°(IQR 6.02)、3.86°(IQR 2.55)、4.81°(IQR 4.37)和4.92°(IQR 3.27)。四个水平的平均位置偏差分别为3.15 mm (IQR 3.54)、3.55 mm (IQR 1.37)、4.26 mm (IQR 2.61)和4.86 mm (IQR 3.93)。不同水平的角度和位置偏差无显著差异。然而,位置偏差> 2 mm和> 5 mm的个体比例在SI关节尾端明显大于上端。位置偏差均在8mm以内。平均随访时间为24.4个月。在最后一次随访中,3例患者出现局部复发,1例患者死于疾病。所有假体均就位,无明显移位。肌肉骨骼肿瘤学会评分系统(MSTS93)和MUD评分(下肢功能和感觉(M)、排尿和输尿管感觉(U)、排便和直肠感觉(D))的平均值分别为19.4(16 ~ 24)和16.3(12 ~ 24)。结论:值得注意的是,3d打印患者特异性手术夹具在全骶骨切除术中具有较高的截骨准确性,并可获得最佳的手术切缘和重建。使用定制的3d打印内假体可以实现有效可靠的重建。通过准确性验证,3D打印技术在全骶骨切除术中应用于患者特异性手术夹具和定制3D打印植入物,具有较高的手术准确性。
How precise is excision and reconstruction using 3D printing technology for total sacrectomy: accuracy validation in 9 consecutive cases.
Background: With 3D printing technology, we can now use preoperative imaging for precise surgical plan. We can also use patient-specific surgical jig to improve the accuracy of osteotomy and 3D-printed custom-made endoprostheses combined with a screw-rod system to restore lumbosacral stability. The aim of this study was to evaluate the accuracy of 3D printing technology for precise osteotomy during total sacrectomy.
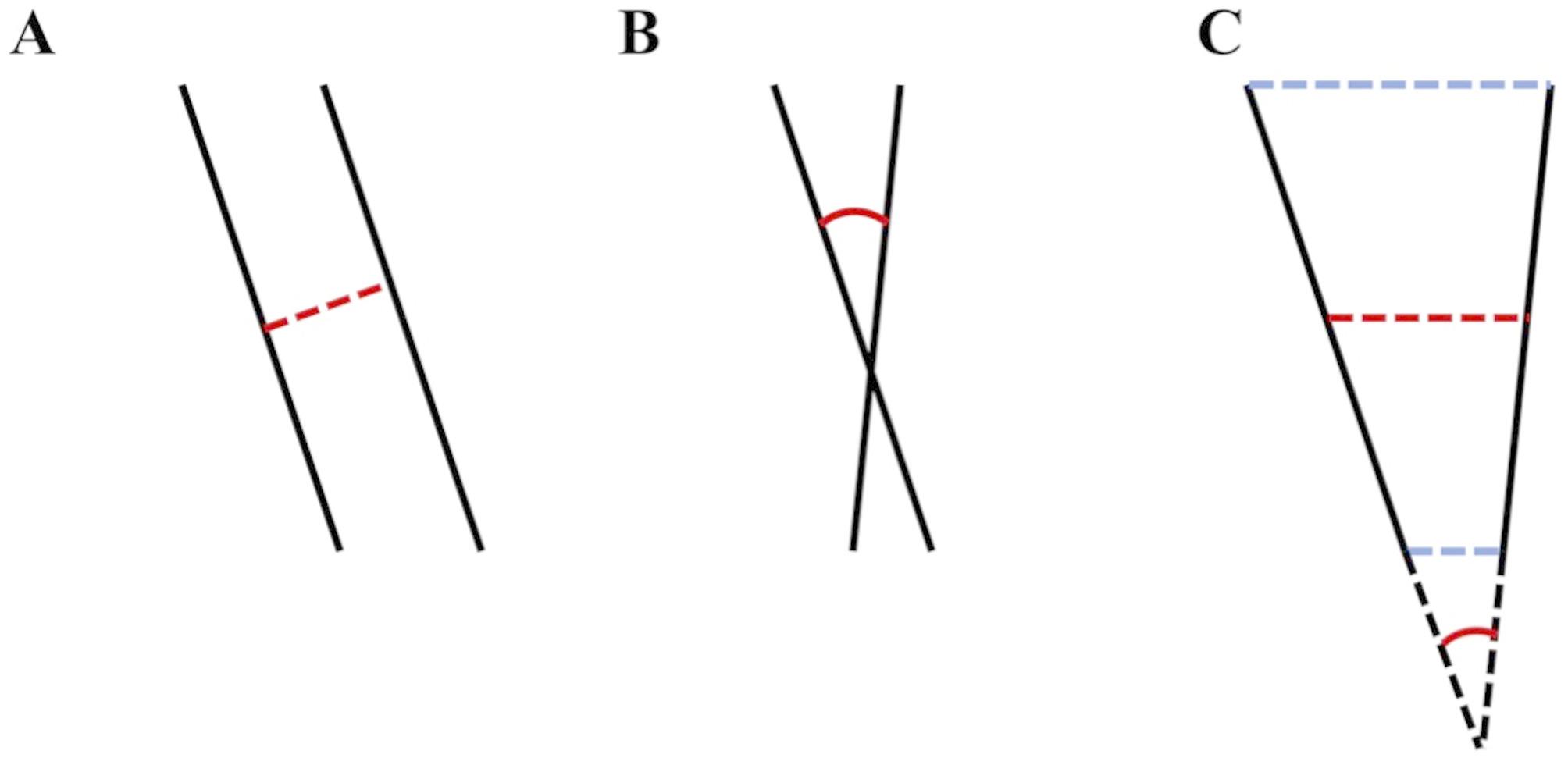
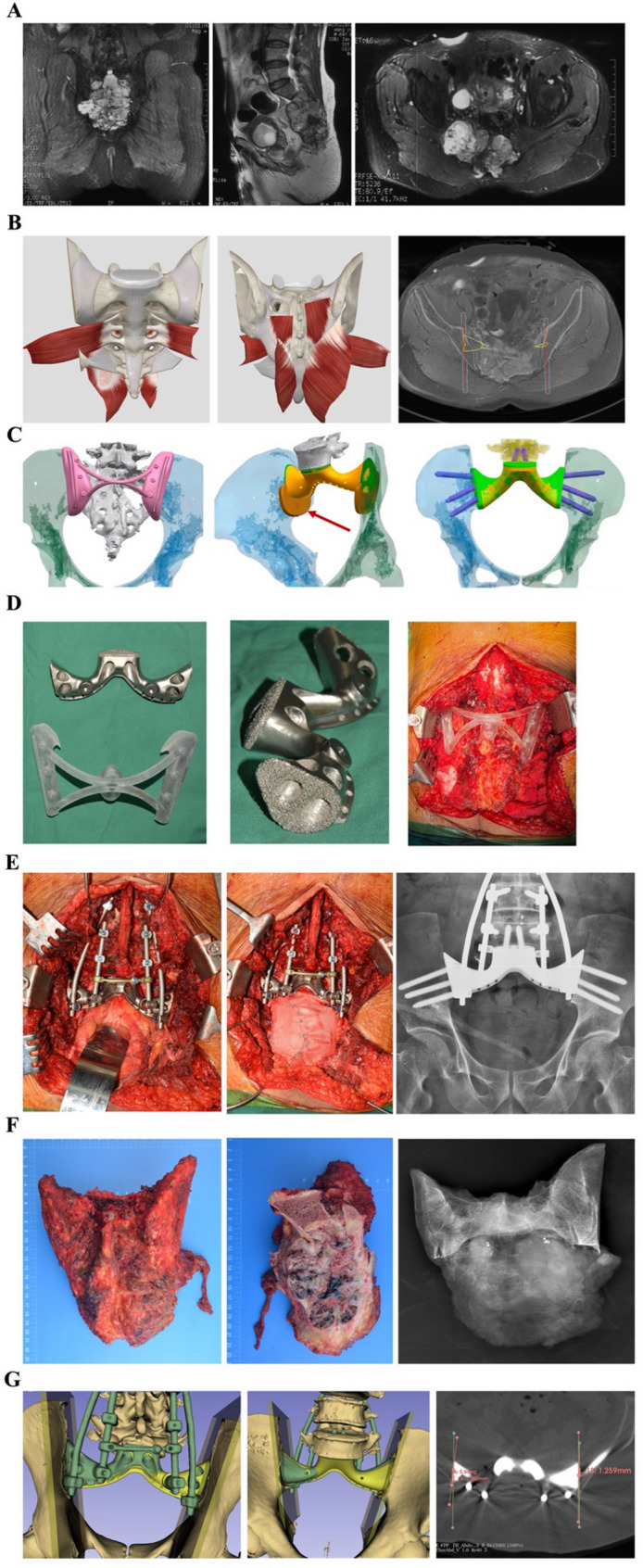
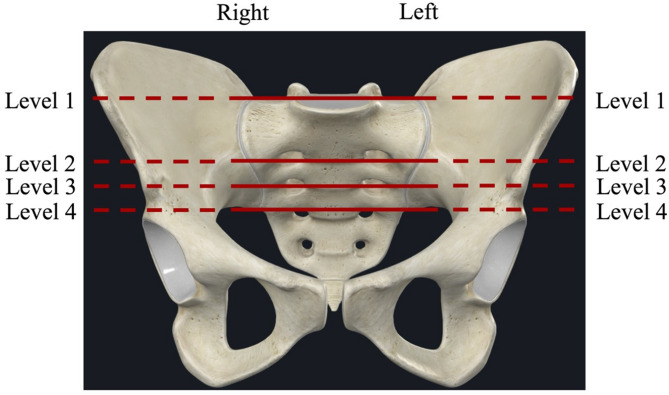
Methods: Nine patients with primary malignant tumors of the sacrum who underwent total sacrectomy at our center were enrolled. Osteotomy was planned based on preoperative imaging (CT, MRI). Generally, an additional 8-10 mm margin beyond the tumor was determined by the fusion of MR and CT images. Patient-specific surgical jigs and 3D-printed sacral endoprostheses were then designed based on the planned osteotomy planes. Pre- and postoperative 3D models of the lumbosacral and pelvic regions were constructed using the fiducial registration model of 3D slicer software 5.1.0. Postoperative CT scans were compared with the planned osteomy planes based on preoperative CT scans, in order to evaluate the accuracy of the osteotomy and endoprosthetic reconstruction. For each patient, four levels of osteotomy planes were chosen, including the upper edge of the sacroiliac (SI) joint, the S1 and S2 foramen levels, and the caudal edge of the SI joint, for analyzing position and angular deviations between the preoperative plan and actual osteotomy along with the endoprosthesis position.
Results: Pathological diagnoses included four cases of osteosarcoma, four cases of chordoma, and one case of Ewing sarcoma. All osteotomies in nine patients achieved R0 resection, as verified pathologically. An average angular deviation of 4.27° (interquartile range[IQR] 4.15) and an osteotomy position deviation of 4.00 mm (IQR 2.90) were observed. The mean angular deviations of the four levels were 3.50° (IQR 6.02), 3.86° (IQR 2.55), 4.81° (IQR 4.37), and 4.92° (IQR 3.27). The mean position deviations at the four levels were 3.15 mm (IQR 3.54), 3.55 mm (IQR 1.37), 4.26 mm (IQR 2.61), and 4.86 mm (IQR 3.93). No significant difference was found among the angular and position deviations at different levels. However, the proportions of individuals with position deviations > 2 mm and > 5 mm were significantly greater at the caudal end of the SI joint than at the upper end. All position deviations were within 8 mm. The average follow-up duration was 24.4 months. At the last follow-up, three patients experienced local recurrence, and one patient died of disease. All endoprostheses were in place without significant displacement. The mean Musculoskeletal Tumor Society scoring system (MSTS93) and MUD scores (function and sensation of lower limbs (M), urination and uriesthesia (U), and defecation and rectal sensation (D)) were 19.4 (16 to 24) and 16.3 (12 to 24), respectively.
Conclusion: Notably, 3D-printed patient-specific surgical jigs exhibit high accuracy of osteotomy and lead to optimal surgical margin and reconstruction in total sacrectomy. Effective and reliable reconstruction can be achieved with a custom-made 3D-printed endoprosthesis. The application of 3D printing technology using patient-specific surgical jigs and the custom-made 3D-printed implants exhibited high surgical accuracy in total sacrectomy, as evidenced by accuracy validation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


