Souvik Maitra, Dalim K Baidya, Bikash R Ray, Choro A Kayina, Damarla Haritha, Parvathy R Nair, Sulagna Bhattacharjee
{"title":"COVID-19患者急性呼吸窘迫综合征全球定义的验证:一项回顾性研究","authors":"Souvik Maitra, Dalim K Baidya, Bikash R Ray, Choro A Kayina, Damarla Haritha, Parvathy R Nair, Sulagna Bhattacharjee","doi":"10.5005/jp-journals-10071-25006","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>A recent acute respiratory distress syndrome (ARDS) definition included patients receiving high-flow nasal oxygen (HFNO) when fulfilling the oxygenation and radiological criteria of ARDS Berlin definition. However, outcome of patients treated may be better than those who fulfilled the corresponding class of Berlin definition. This study was aimed to compare the survival between patients fulfilling Berlin definition and patients managed by HFNO initially.</p><p><strong>Patients and methods: </strong>Patients fulfilling the World Health Organization case definition of severe or critical COVID-19 infection requiring HFNO (at least 30 L/minute of flow), noninvasive ventilation (NIV) (at least a positive end-expiratory pressure (PEEP) of 5 cm H<sub>2</sub>O), or invasive mechanical ventilation (at least a PEEP of 5 cm H<sub>2</sub>O) were included in this study provided they fulfilled oxygenation and radiological criteria of ARDS as per Berlin definition.</p><p><strong>Results: </strong>All-cause hospital mortality rate in patients who fulfilled Berlin definition (<i>n</i> = 193) was 47.6% (mild ARDS), 64.9% (moderate ARDS), and 67.9% (severe ARDS) (<i>p</i> = 0.23). Multivariable survival analysis reported that hazard of death was higher in patients who fulfilled Berlin definition as opposed to those who were initially managed by HFNO (adjusted hazard ratio (95% confidence interval) 1.68 (1.15-2.45), <i>p</i> = 0.007) after adjustment for age, Charlson comorbidity index, and baseline PaO<sub>2</sub>/FiO<sub>2</sub> ratio. Multiple pairwise comparison reported that hazard of death was lower in patients with moderate ARDS requiring HFNO as compared with the moderate ARDS patients as per Berlin definition (<i>p</i> = 0.024). However, no difference was observed in patients of mild (<i>p</i> = 0.39) and severe ARDS (<i>p</i> = 0.24).</p><p><strong>Conclusion: </strong>We have found a statistically significant higher survival in ARDS patients managed by HFNO in the first 24 hours after intensive care unit (ICU) admission when compared with the patients receiving NIV or invasive mechanical ventilation. So, we conclude that outcome of patients fulfilling the global definition of ARDS is largely different from those who fulfilled Berlin definition. Hence, prospective multicentric validation is required before its bedside use.</p><p><strong>How to cite this article: </strong>Maitra S, Baidya DK, Ray BR, Kayina CA, Haritha D, Nair PR, <i>et al</i>. Validation of Global Definition of Acute Respiratory Distress Syndrome in COVID-19 Patients: A Retrospective Study. Indian J Crit Care Med 2025;29(7):556-561.</p>","PeriodicalId":47664,"journal":{"name":"Indian Journal of Critical Care Medicine","volume":"29 7","pages":"556-561"},"PeriodicalIF":1.5000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12302224/pdf/","citationCount":"0","resultStr":"{\"title\":\"Validation of Global Definition of Acute Respiratory Distress Syndrome in COVID-19 Patients: A Retrospective Study.\",\"authors\":\"Souvik Maitra, Dalim K Baidya, Bikash R Ray, Choro A Kayina, Damarla Haritha, Parvathy R Nair, Sulagna Bhattacharjee\",\"doi\":\"10.5005/jp-journals-10071-25006\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and aims: </strong>A recent acute respiratory distress syndrome (ARDS) definition included patients receiving high-flow nasal oxygen (HFNO) when fulfilling the oxygenation and radiological criteria of ARDS Berlin definition. However, outcome of patients treated may be better than those who fulfilled the corresponding class of Berlin definition. This study was aimed to compare the survival between patients fulfilling Berlin definition and patients managed by HFNO initially.</p><p><strong>Patients and methods: </strong>Patients fulfilling the World Health Organization case definition of severe or critical COVID-19 infection requiring HFNO (at least 30 L/minute of flow), noninvasive ventilation (NIV) (at least a positive end-expiratory pressure (PEEP) of 5 cm H<sub>2</sub>O), or invasive mechanical ventilation (at least a PEEP of 5 cm H<sub>2</sub>O) were included in this study provided they fulfilled oxygenation and radiological criteria of ARDS as per Berlin definition.</p><p><strong>Results: </strong>All-cause hospital mortality rate in patients who fulfilled Berlin definition (<i>n</i> = 193) was 47.6% (mild ARDS), 64.9% (moderate ARDS), and 67.9% (severe ARDS) (<i>p</i> = 0.23). Multivariable survival analysis reported that hazard of death was higher in patients who fulfilled Berlin definition as opposed to those who were initially managed by HFNO (adjusted hazard ratio (95% confidence interval) 1.68 (1.15-2.45), <i>p</i> = 0.007) after adjustment for age, Charlson comorbidity index, and baseline PaO<sub>2</sub>/FiO<sub>2</sub> ratio. Multiple pairwise comparison reported that hazard of death was lower in patients with moderate ARDS requiring HFNO as compared with the moderate ARDS patients as per Berlin definition (<i>p</i> = 0.024). However, no difference was observed in patients of mild (<i>p</i> = 0.39) and severe ARDS (<i>p</i> = 0.24).</p><p><strong>Conclusion: </strong>We have found a statistically significant higher survival in ARDS patients managed by HFNO in the first 24 hours after intensive care unit (ICU) admission when compared with the patients receiving NIV or invasive mechanical ventilation. So, we conclude that outcome of patients fulfilling the global definition of ARDS is largely different from those who fulfilled Berlin definition. Hence, prospective multicentric validation is required before its bedside use.</p><p><strong>How to cite this article: </strong>Maitra S, Baidya DK, Ray BR, Kayina CA, Haritha D, Nair PR, <i>et al</i>. Validation of Global Definition of Acute Respiratory Distress Syndrome in COVID-19 Patients: A Retrospective Study. Indian J Crit Care Med 2025;29(7):556-561.</p>\",\"PeriodicalId\":47664,\"journal\":{\"name\":\"Indian Journal of Critical Care Medicine\",\"volume\":\"29 7\",\"pages\":\"556-561\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12302224/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Indian Journal of Critical Care Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5005/jp-journals-10071-25006\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Critical Care Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5005/jp-journals-10071-25006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景和目的:最近的急性呼吸窘迫综合征(ARDS)定义包括在满足ARDS柏林定义的氧合和放射学标准时接受高流量鼻吸氧(HFNO)的患者。然而,接受治疗的患者的预后可能优于符合柏林定义的相应类别的患者。本研究旨在比较符合柏林定义的患者和最初采用HFNO治疗的患者的生存率。患者和方法:符合世界卫生组织病例定义的重症或危重型COVID-19感染患者需要HFNO(至少30 L/min的流量)、无创通气(至少5 cm H2O的呼气末正压(PEEP))或有创机械通气(至少5 cm H2O的PEEP),只要他们符合柏林定义的ARDS的氧合和放射学标准,就被纳入本研究。结果:符合柏林定义的患者(n = 193)的全因住院死亡率分别为47.6%(轻度ARDS)、64.9%(中度ARDS)和67.9%(重度ARDS) (p = 0.23)。多变量生存分析报告,在调整年龄、Charlson合病指数和基线PaO2/FiO2比后,符合柏林定义的患者的死亡风险高于最初接受HFNO治疗的患者(校正风险比(95%置信区间)1.68 (1.15-2.45),p = 0.007)。多成对比较报道,根据柏林定义,需要HFNO的中度ARDS患者的死亡风险低于中度ARDS患者(p = 0.024)。然而,轻度(p = 0.39)和重度(p = 0.24) ARDS患者的差异无统计学意义。结论:我们发现HFNO治疗的ARDS患者在重症监护病房(ICU)入院后24小时内的生存率明显高于接受无创通气或有创机械通气的患者。因此,我们得出结论,满足ARDS全球定义的患者的结局与满足柏林定义的患者有很大不同。因此,在临床应用前需要进行前瞻性多中心验证。如何引用:Maitra S, Baidya DK, Ray BR, Kayina CA, Haritha D, Nair PR等。COVID-19患者急性呼吸窘迫综合征全球定义的验证:一项回顾性研究中华检验医学杂志;2015;29(7):556-561。
Validation of Global Definition of Acute Respiratory Distress Syndrome in COVID-19 Patients: A Retrospective Study.
Background and aims: A recent acute respiratory distress syndrome (ARDS) definition included patients receiving high-flow nasal oxygen (HFNO) when fulfilling the oxygenation and radiological criteria of ARDS Berlin definition. However, outcome of patients treated may be better than those who fulfilled the corresponding class of Berlin definition. This study was aimed to compare the survival between patients fulfilling Berlin definition and patients managed by HFNO initially.
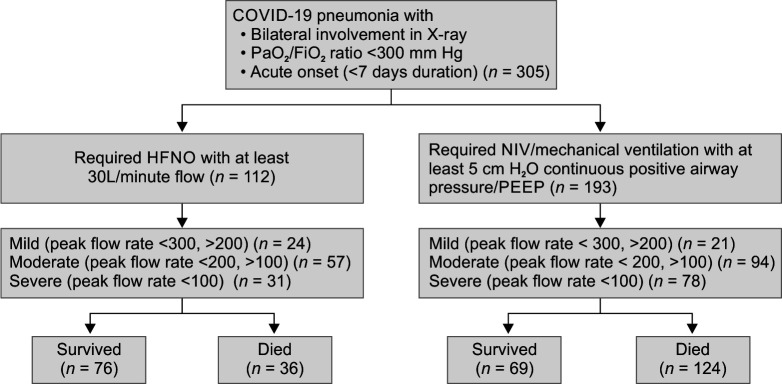
Patients and methods: Patients fulfilling the World Health Organization case definition of severe or critical COVID-19 infection requiring HFNO (at least 30 L/minute of flow), noninvasive ventilation (NIV) (at least a positive end-expiratory pressure (PEEP) of 5 cm H2O), or invasive mechanical ventilation (at least a PEEP of 5 cm H2O) were included in this study provided they fulfilled oxygenation and radiological criteria of ARDS as per Berlin definition.
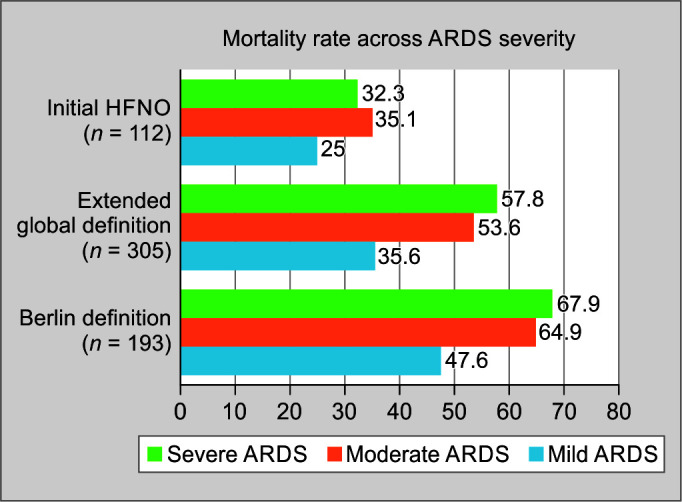
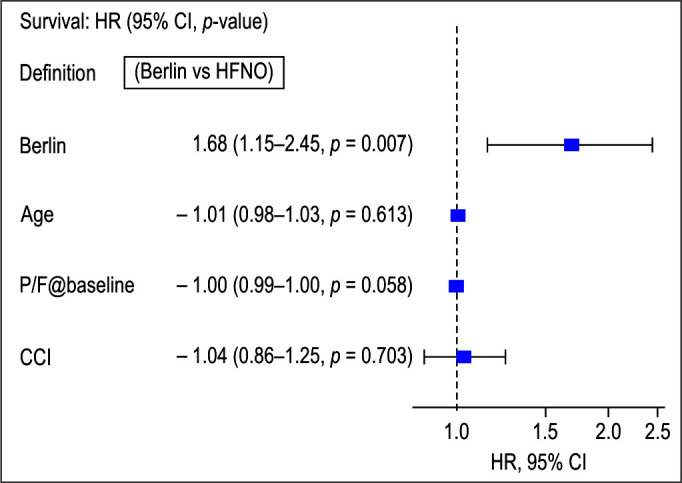
Results: All-cause hospital mortality rate in patients who fulfilled Berlin definition (n = 193) was 47.6% (mild ARDS), 64.9% (moderate ARDS), and 67.9% (severe ARDS) (p = 0.23). Multivariable survival analysis reported that hazard of death was higher in patients who fulfilled Berlin definition as opposed to those who were initially managed by HFNO (adjusted hazard ratio (95% confidence interval) 1.68 (1.15-2.45), p = 0.007) after adjustment for age, Charlson comorbidity index, and baseline PaO2/FiO2 ratio. Multiple pairwise comparison reported that hazard of death was lower in patients with moderate ARDS requiring HFNO as compared with the moderate ARDS patients as per Berlin definition (p = 0.024). However, no difference was observed in patients of mild (p = 0.39) and severe ARDS (p = 0.24).
Conclusion: We have found a statistically significant higher survival in ARDS patients managed by HFNO in the first 24 hours after intensive care unit (ICU) admission when compared with the patients receiving NIV or invasive mechanical ventilation. So, we conclude that outcome of patients fulfilling the global definition of ARDS is largely different from those who fulfilled Berlin definition. Hence, prospective multicentric validation is required before its bedside use.
How to cite this article: Maitra S, Baidya DK, Ray BR, Kayina CA, Haritha D, Nair PR, et al. Validation of Global Definition of Acute Respiratory Distress Syndrome in COVID-19 Patients: A Retrospective Study. Indian J Crit Care Med 2025;29(7):556-561.
期刊介绍:
Indian Journal of Critical Care Medicine (ISSN 0972-5229) is specialty periodical published under the auspices of Indian Society of Critical Care Medicine. Journal encourages research, education and dissemination of knowledge in the fields of critical and emergency medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


