Nabil Al Shammas, Robert Luck, Sophie Schumann, Dragana Köhler, Lutz Mirow, Bernhard Rosengarten
{"title":"极度肥胖患者颅内压水平的临界上移由于减肥手术而恢复正常。","authors":"Nabil Al Shammas, Robert Luck, Sophie Schumann, Dragana Köhler, Lutz Mirow, Bernhard Rosengarten","doi":"10.1186/s13089-025-00439-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Increase in body mass index (BMI) is a risk factor for idiopathic intracranial hypertension (IIH). The matter of body weight and intracranial pressure (ICP) in clinically asymptomatic obese patients is unknown. We aimed at studying the relationship of ICP and BMI pre- and post-surgery in obese patients undergoing bariatric surgery.</p><p><strong>Methods: </strong>Patients with a BMI > 35 kg/m<sup>2</sup>, qualified for bariatric surgery and without clinical signs of IIH were prospectively and consecutively included. The optic nerve sheath diameter (ONSD) and a combined transcranial Doppler-arterial blood pressure (TCD&ABP-ICP) method were used to non-invasively determine the ICP (nICP) pre- and post-surgery (six months after surgery when weight loss had stabilized). ONSD > 5.8 mm and nICP > 25cmH<sub>2</sub>O were assumed as pathologically increased. A nICP between > 20 and ≤ 25 cmH2O was assumed as being in the borderline.</p><p><strong>Results: </strong>54 patients (43 female; 44 ± 11 years old) were included. Pre-surgery BMI (46 ± 6 kg/m<sup>2</sup>) significantly declined after surgery (post-surgery BMI: 32 ± 6 kg/m2; paired t-test: p < 0.0001). Initial ONSD was 5.8 ± 0.6 mm (6 pathological values) which declined to 5.4 ± 0.6 mm (5 pathological values) (paired t-test: p < 0.025). TCD&ABP assessed nICP was 19 ± 4.5 cmH<sub>2</sub>O (5 with pathological, 16 with borderline values) pre-surgically and declined to 14 ± 4 cmH<sub>2</sub>O (no pathological, 1 high-normal value) after surgery (p < 0.0001).</p><p><strong>Conclusion: </strong>Assuming the low incidence of IIH, the frequency of pathologic and borderline ICP values in obese patients was unexpectedly high. Reduction of ICP with weight loss followed a simple regression line pointing to a mechanistic effect of increased body weight on ICP. The constancy of pathologic ONSD values might be due to a fixed dilatation of the optic nerve sheath due to the duration of obesity.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":"17 1","pages":"35"},"PeriodicalIF":2.9000,"publicationDate":"2025-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12304339/pdf/","citationCount":"0","resultStr":"{\"title\":\"Critical upward shift of intracranial pressure levels in extremely obese patients; normalization due to bariatric surgery.\",\"authors\":\"Nabil Al Shammas, Robert Luck, Sophie Schumann, Dragana Köhler, Lutz Mirow, Bernhard Rosengarten\",\"doi\":\"10.1186/s13089-025-00439-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Increase in body mass index (BMI) is a risk factor for idiopathic intracranial hypertension (IIH). The matter of body weight and intracranial pressure (ICP) in clinically asymptomatic obese patients is unknown. We aimed at studying the relationship of ICP and BMI pre- and post-surgery in obese patients undergoing bariatric surgery.</p><p><strong>Methods: </strong>Patients with a BMI > 35 kg/m<sup>2</sup>, qualified for bariatric surgery and without clinical signs of IIH were prospectively and consecutively included. The optic nerve sheath diameter (ONSD) and a combined transcranial Doppler-arterial blood pressure (TCD&ABP-ICP) method were used to non-invasively determine the ICP (nICP) pre- and post-surgery (six months after surgery when weight loss had stabilized). ONSD > 5.8 mm and nICP > 25cmH<sub>2</sub>O were assumed as pathologically increased. A nICP between > 20 and ≤ 25 cmH2O was assumed as being in the borderline.</p><p><strong>Results: </strong>54 patients (43 female; 44 ± 11 years old) were included. Pre-surgery BMI (46 ± 6 kg/m<sup>2</sup>) significantly declined after surgery (post-surgery BMI: 32 ± 6 kg/m2; paired t-test: p < 0.0001). Initial ONSD was 5.8 ± 0.6 mm (6 pathological values) which declined to 5.4 ± 0.6 mm (5 pathological values) (paired t-test: p < 0.025). TCD&ABP assessed nICP was 19 ± 4.5 cmH<sub>2</sub>O (5 with pathological, 16 with borderline values) pre-surgically and declined to 14 ± 4 cmH<sub>2</sub>O (no pathological, 1 high-normal value) after surgery (p < 0.0001).</p><p><strong>Conclusion: </strong>Assuming the low incidence of IIH, the frequency of pathologic and borderline ICP values in obese patients was unexpectedly high. Reduction of ICP with weight loss followed a simple regression line pointing to a mechanistic effect of increased body weight on ICP. The constancy of pathologic ONSD values might be due to a fixed dilatation of the optic nerve sheath due to the duration of obesity.</p>\",\"PeriodicalId\":36911,\"journal\":{\"name\":\"Ultrasound Journal\",\"volume\":\"17 1\",\"pages\":\"35\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-07-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12304339/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ultrasound Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13089-025-00439-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-025-00439-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Critical upward shift of intracranial pressure levels in extremely obese patients; normalization due to bariatric surgery.
Background: Increase in body mass index (BMI) is a risk factor for idiopathic intracranial hypertension (IIH). The matter of body weight and intracranial pressure (ICP) in clinically asymptomatic obese patients is unknown. We aimed at studying the relationship of ICP and BMI pre- and post-surgery in obese patients undergoing bariatric surgery.
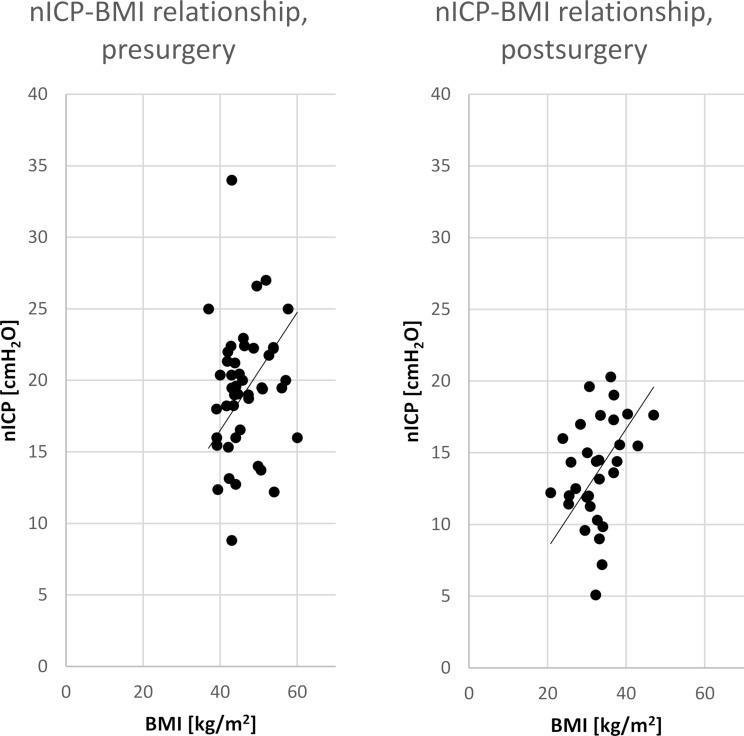
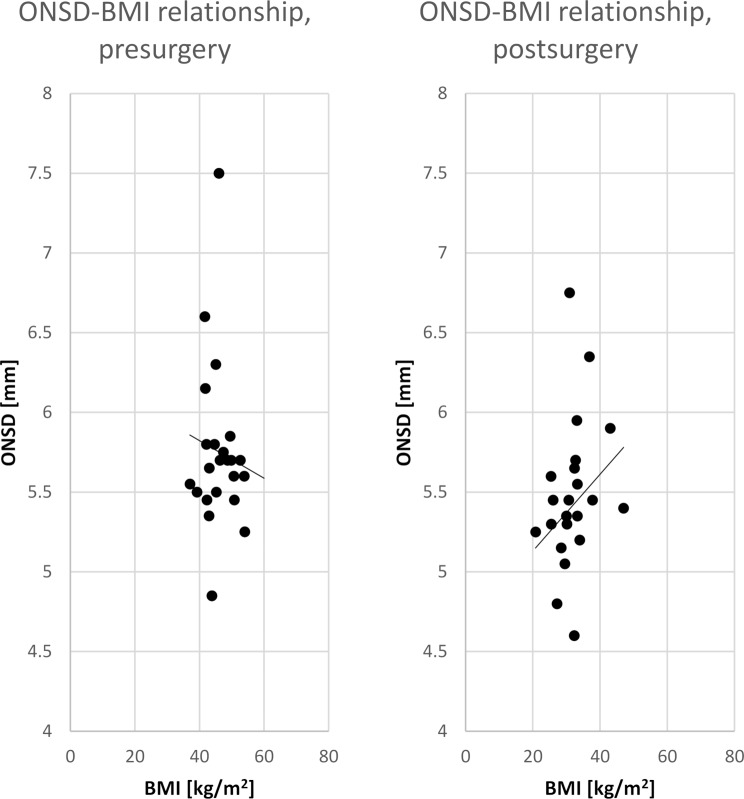
Methods: Patients with a BMI > 35 kg/m2, qualified for bariatric surgery and without clinical signs of IIH were prospectively and consecutively included. The optic nerve sheath diameter (ONSD) and a combined transcranial Doppler-arterial blood pressure (TCD&ABP-ICP) method were used to non-invasively determine the ICP (nICP) pre- and post-surgery (six months after surgery when weight loss had stabilized). ONSD > 5.8 mm and nICP > 25cmH2O were assumed as pathologically increased. A nICP between > 20 and ≤ 25 cmH2O was assumed as being in the borderline.
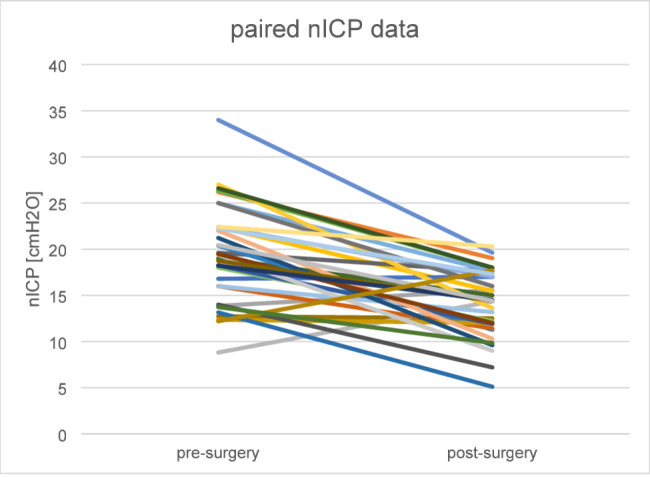
Results: 54 patients (43 female; 44 ± 11 years old) were included. Pre-surgery BMI (46 ± 6 kg/m2) significantly declined after surgery (post-surgery BMI: 32 ± 6 kg/m2; paired t-test: p < 0.0001). Initial ONSD was 5.8 ± 0.6 mm (6 pathological values) which declined to 5.4 ± 0.6 mm (5 pathological values) (paired t-test: p < 0.025). TCD&ABP assessed nICP was 19 ± 4.5 cmH2O (5 with pathological, 16 with borderline values) pre-surgically and declined to 14 ± 4 cmH2O (no pathological, 1 high-normal value) after surgery (p < 0.0001).
Conclusion: Assuming the low incidence of IIH, the frequency of pathologic and borderline ICP values in obese patients was unexpectedly high. Reduction of ICP with weight loss followed a simple regression line pointing to a mechanistic effect of increased body weight on ICP. The constancy of pathologic ONSD values might be due to a fixed dilatation of the optic nerve sheath due to the duration of obesity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


