{"title":"早期强化治疗预防分支动脉粥样硬化性疾病的神经功能恶化。","authors":"Yen-Chu Huang, Hsu-Huei Weng, Yuan-Hsiung Tsai, Leng-Chieh Lin, Jiann-Der Lee, Jen-Tsung Yang, Yi-Ting Pan","doi":"10.1177/17562864251357274","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Branch atheromatous disease (BAD) is a subtype of ischemic stroke associated with early neurological deterioration (END) and poor outcomes. Although BAD shares features with large artery atherosclerosis, optimal treatment strategies remain undefined.</p><p><strong>Objectives: </strong>To assess the efficacy and safety of early dual antiplatelet therapy (DAPT) and high-intensity statins in reducing END and improving outcomes in BAD.</p><p><strong>Design: </strong>A prospective, single-arm study with a historical control group.</p><p><strong>Methods: </strong>This study reports the results of the Statin and Dual Antiplatelet Therapy in Preventing Early Neurological Deterioration in Branch Atheromatous Disease trial. Patients with BAD-related ischemic stroke were treated with aspirin, clopidogrel, and high-intensity statins within 24 h of symptom onset. Outcomes were compared with a historical control cohort treated with single antiplatelet therapy and moderate- or low-intensity statins. The primary outcome was the composite of END (defined as an National Institutes of Health Stroke Scale score increase ⩾2 points within 7 days) or recurrent stroke within 30 days. Secondary outcomes included severe END, functional outcomes at 90 days, and safety events.</p><p><strong>Results: </strong>A total of 91 patients received intensive therapy and 285 received standard treatment. The primary endpoint occurred less frequently in the intensive group (34.1% vs 48.1%; adjusted risk ratio (aRR), 0.71; 95% confidence interval (CI), 0.52-0.98; <i>p</i> = 0.034). Intensive therapy significantly reduced END at 7 days (34.1% vs 47.0%; aRR, 0.73; 95% CI, 0.54-1.00; <i>p</i> = 0.049) but not recurrent stroke at 30 days (2.2% vs 1.8%; aRR, 1.16; 95% CI, 0.25-5.43). Good outcomes at 90 days (modified Rankin Scale ⩽2) were more common with intensive therapy (73.6% vs 57.2%; aRR, 1.27; 95% CI, 1.09-1.48; <i>p</i> = 0.002). Major bleeding and mortality did not differ between groups.</p><p><strong>Conclusion: </strong>Early intensive therapy with DAPT and high-intensity statins significantly reduced END and improved recovery in BAD without compromising safety. Further studies are warranted to validate these findings.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov; Identifier: NCT04824911 (https://clinicaltrials.gov/study/NCT04824911).</p>","PeriodicalId":22980,"journal":{"name":"Therapeutic Advances in Neurological Disorders","volume":"18 ","pages":"17562864251357274"},"PeriodicalIF":4.1000,"publicationDate":"2025-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12301609/pdf/","citationCount":"0","resultStr":"{\"title\":\"Early intensive therapy for preventing neurological deterioration in branch atheromatous disease.\",\"authors\":\"Yen-Chu Huang, Hsu-Huei Weng, Yuan-Hsiung Tsai, Leng-Chieh Lin, Jiann-Der Lee, Jen-Tsung Yang, Yi-Ting Pan\",\"doi\":\"10.1177/17562864251357274\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Branch atheromatous disease (BAD) is a subtype of ischemic stroke associated with early neurological deterioration (END) and poor outcomes. Although BAD shares features with large artery atherosclerosis, optimal treatment strategies remain undefined.</p><p><strong>Objectives: </strong>To assess the efficacy and safety of early dual antiplatelet therapy (DAPT) and high-intensity statins in reducing END and improving outcomes in BAD.</p><p><strong>Design: </strong>A prospective, single-arm study with a historical control group.</p><p><strong>Methods: </strong>This study reports the results of the Statin and Dual Antiplatelet Therapy in Preventing Early Neurological Deterioration in Branch Atheromatous Disease trial. Patients with BAD-related ischemic stroke were treated with aspirin, clopidogrel, and high-intensity statins within 24 h of symptom onset. Outcomes were compared with a historical control cohort treated with single antiplatelet therapy and moderate- or low-intensity statins. The primary outcome was the composite of END (defined as an National Institutes of Health Stroke Scale score increase ⩾2 points within 7 days) or recurrent stroke within 30 days. Secondary outcomes included severe END, functional outcomes at 90 days, and safety events.</p><p><strong>Results: </strong>A total of 91 patients received intensive therapy and 285 received standard treatment. The primary endpoint occurred less frequently in the intensive group (34.1% vs 48.1%; adjusted risk ratio (aRR), 0.71; 95% confidence interval (CI), 0.52-0.98; <i>p</i> = 0.034). Intensive therapy significantly reduced END at 7 days (34.1% vs 47.0%; aRR, 0.73; 95% CI, 0.54-1.00; <i>p</i> = 0.049) but not recurrent stroke at 30 days (2.2% vs 1.8%; aRR, 1.16; 95% CI, 0.25-5.43). Good outcomes at 90 days (modified Rankin Scale ⩽2) were more common with intensive therapy (73.6% vs 57.2%; aRR, 1.27; 95% CI, 1.09-1.48; <i>p</i> = 0.002). Major bleeding and mortality did not differ between groups.</p><p><strong>Conclusion: </strong>Early intensive therapy with DAPT and high-intensity statins significantly reduced END and improved recovery in BAD without compromising safety. Further studies are warranted to validate these findings.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov; Identifier: NCT04824911 (https://clinicaltrials.gov/study/NCT04824911).</p>\",\"PeriodicalId\":22980,\"journal\":{\"name\":\"Therapeutic Advances in Neurological Disorders\",\"volume\":\"18 \",\"pages\":\"17562864251357274\"},\"PeriodicalIF\":4.1000,\"publicationDate\":\"2025-07-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12301609/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Neurological Disorders\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17562864251357274\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Neurological Disorders","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562864251357274","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:分支动脉粥样硬化疾病(BAD)是缺血性卒中的一种亚型,与早期神经功能恶化(END)和不良预后相关。尽管BAD与大动脉粥样硬化有相同的特征,但最佳治疗策略仍不明确。目的:评估早期双重抗血小板治疗(DAPT)和高强度他汀类药物在减少END和改善BAD预后方面的有效性和安全性。设计:前瞻性单臂研究,有历史对照组。方法:本研究报告了他汀类药物联合双重抗血小板治疗预防分支动脉粥样硬化疾病早期神经功能恶化的试验结果。bad相关缺血性脑卒中患者在症状出现24小时内给予阿司匹林、氯吡格雷和高强度他汀类药物治疗。结果与单一抗血小板治疗和中低强度他汀类药物治疗的历史对照队列进行比较。主要结果是END(定义为7天内美国国立卫生研究院卒中量表评分增加大于或等于2分)或30天内复发性卒中的综合结果。次要结局包括严重的END、90天的功能结局和安全事件。结果:强化治疗91例,标准治疗285例。强化组的主要终点发生频率较低(34.1% vs 48.1%;调整风险比(aRR), 0.71;95%置信区间(CI), 0.52-0.98;p = 0.034)。强化治疗显著降低7天END (34.1% vs 47.0%;加勒比海盗,0.73;95% ci, 0.54-1.00;P = 0.049),但30天无卒中复发(2.2% vs 1.8%;加勒比海盗,1.16;95% ci, 0.25-5.43)。90天的良好预后(改良Rankin量表≥2)在强化治疗中更为常见(73.6% vs 57.2%;加勒比海盗,1.27;95% ci, 1.09-1.48;p = 0.002)。大出血和死亡率在两组之间没有差异。结论:DAPT和高强度他汀类药物的早期强化治疗可显著降低BAD的END并改善其恢复,同时不影响安全性。需要进一步的研究来证实这些发现。试验注册:ClinicalTrials.gov;标识符:NCT04824911 (https://clinicaltrials.gov/study/NCT04824911)。
Early intensive therapy for preventing neurological deterioration in branch atheromatous disease.
Background: Branch atheromatous disease (BAD) is a subtype of ischemic stroke associated with early neurological deterioration (END) and poor outcomes. Although BAD shares features with large artery atherosclerosis, optimal treatment strategies remain undefined.
Objectives: To assess the efficacy and safety of early dual antiplatelet therapy (DAPT) and high-intensity statins in reducing END and improving outcomes in BAD.
Design: A prospective, single-arm study with a historical control group.
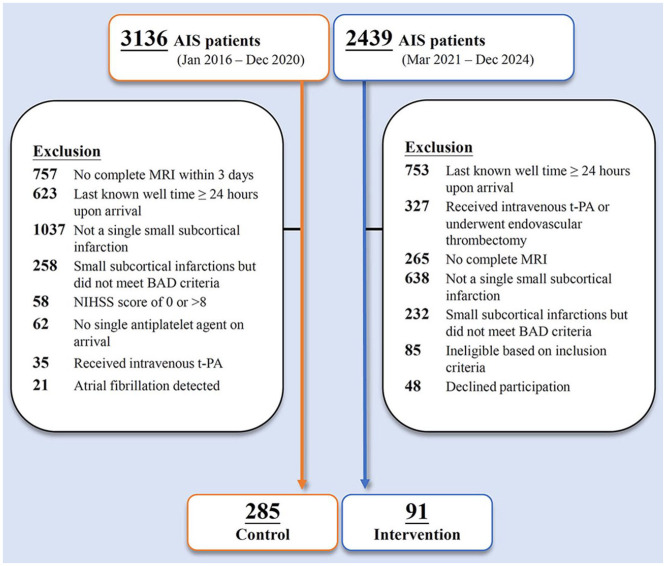
Methods: This study reports the results of the Statin and Dual Antiplatelet Therapy in Preventing Early Neurological Deterioration in Branch Atheromatous Disease trial. Patients with BAD-related ischemic stroke were treated with aspirin, clopidogrel, and high-intensity statins within 24 h of symptom onset. Outcomes were compared with a historical control cohort treated with single antiplatelet therapy and moderate- or low-intensity statins. The primary outcome was the composite of END (defined as an National Institutes of Health Stroke Scale score increase ⩾2 points within 7 days) or recurrent stroke within 30 days. Secondary outcomes included severe END, functional outcomes at 90 days, and safety events.
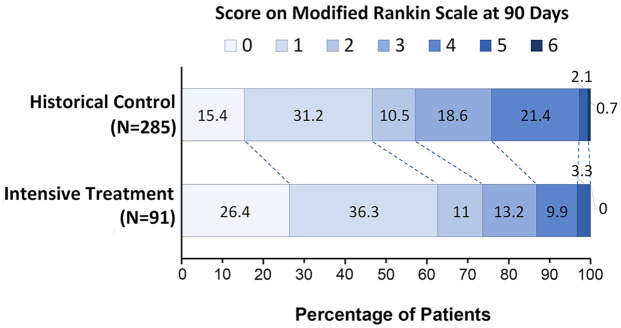
Results: A total of 91 patients received intensive therapy and 285 received standard treatment. The primary endpoint occurred less frequently in the intensive group (34.1% vs 48.1%; adjusted risk ratio (aRR), 0.71; 95% confidence interval (CI), 0.52-0.98; p = 0.034). Intensive therapy significantly reduced END at 7 days (34.1% vs 47.0%; aRR, 0.73; 95% CI, 0.54-1.00; p = 0.049) but not recurrent stroke at 30 days (2.2% vs 1.8%; aRR, 1.16; 95% CI, 0.25-5.43). Good outcomes at 90 days (modified Rankin Scale ⩽2) were more common with intensive therapy (73.6% vs 57.2%; aRR, 1.27; 95% CI, 1.09-1.48; p = 0.002). Major bleeding and mortality did not differ between groups.
Conclusion: Early intensive therapy with DAPT and high-intensity statins significantly reduced END and improved recovery in BAD without compromising safety. Further studies are warranted to validate these findings.
期刊介绍:
Therapeutic Advances in Neurological Disorders is a peer-reviewed, open access journal delivering the highest quality articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of neurology. The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in neurology, providing a forum in print and online for publishing the highest quality articles in this area.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


