Philip R Harvey, Richard Rj Wilkin, Shahd A Mohamed, Sarah Powell-Brett, Siobhan C McKay, Georgia R Layton, Keith Roberts, Nigel Trudgill
{"title":"胆道引流治疗恶性胆道梗阻的结果和并发症:全国前瞻性研究。","authors":"Philip R Harvey, Richard Rj Wilkin, Shahd A Mohamed, Sarah Powell-Brett, Siobhan C McKay, Georgia R Layton, Keith Roberts, Nigel Trudgill","doi":"10.1055/a-2558-6754","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and study aims: </strong>National data suggest that biliary drainage for malignant obstruction is associated with high complication rates and early mortality. This study examined factors associated with poor outcomes.</p><p><strong>Patients and methods: </strong>RICOCHET was a national, prospective audit of patients with pancreatic cancer or malignant biliary obstruction between April and August 2018. This analysis reviewed outcomes including complications within 7 days and 30-day mortality following biliary drainage and associated factors.</p><p><strong>Results: </strong>Biliary drainage was attempted in 773 patients, of which, 78.7% were successful at first attempt; but if unsuccessful, only 37% of subsequent attempts succeeded. Complications occurred following 11% of endoscopic retrograde cholangiopancreatographies (ERCPs) (including pancreatitis, 5%) and 12% of percutaneous transhepatic biliary drainages (PTBDs) (including cholangitis, 8%). Complications were associated with: potentially resectable cancer (odds ratio [OR] 1.93, 95% confidence interval [CI] 1.23-3.03); more than one biliary drainage attempt (OR 1.69, 95% CI 1.04-2.74); cholangiocarcinoma (OR 2.20, 95% CI 1.20-4.05), or radiological cancer diagnosis (OR 2.02, 95% CI 1.13-3.60). Thirty-day mortality rates following ERCP and PTBD were 21.4% and 21.4%, respectively, in unresectable cancer and 6% and 6.3%, respectively, in potentially resectable cancer. Increased 30-day mortality in patients with unresectable disease was associated with a performance status of 2 or more (HR 3.14 (1.65-5.97)). Thirty-day mortality was significantly higher in patients with unresectable cancer if a multidisciplinary team meeting had not reviewed and advised drainage prior to the procedure 50% vs 20.4% ( <i>P</i> = 0.028).</p><p><strong>Conclusions: </strong>Careful multidisciplinary consideration of risks and potential benefits should be undertaken prior to attempting malignant biliary drainage due to the high risk of complications and early mortality.</p>","PeriodicalId":11671,"journal":{"name":"Endoscopy International Open","volume":"13 ","pages":"a25586754"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303028/pdf/","citationCount":"0","resultStr":"{\"title\":\"Outcomes and complications of biliary drainage for malignant biliary obstruction: National prospective study.\",\"authors\":\"Philip R Harvey, Richard Rj Wilkin, Shahd A Mohamed, Sarah Powell-Brett, Siobhan C McKay, Georgia R Layton, Keith Roberts, Nigel Trudgill\",\"doi\":\"10.1055/a-2558-6754\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and study aims: </strong>National data suggest that biliary drainage for malignant obstruction is associated with high complication rates and early mortality. This study examined factors associated with poor outcomes.</p><p><strong>Patients and methods: </strong>RICOCHET was a national, prospective audit of patients with pancreatic cancer or malignant biliary obstruction between April and August 2018. This analysis reviewed outcomes including complications within 7 days and 30-day mortality following biliary drainage and associated factors.</p><p><strong>Results: </strong>Biliary drainage was attempted in 773 patients, of which, 78.7% were successful at first attempt; but if unsuccessful, only 37% of subsequent attempts succeeded. Complications occurred following 11% of endoscopic retrograde cholangiopancreatographies (ERCPs) (including pancreatitis, 5%) and 12% of percutaneous transhepatic biliary drainages (PTBDs) (including cholangitis, 8%). Complications were associated with: potentially resectable cancer (odds ratio [OR] 1.93, 95% confidence interval [CI] 1.23-3.03); more than one biliary drainage attempt (OR 1.69, 95% CI 1.04-2.74); cholangiocarcinoma (OR 2.20, 95% CI 1.20-4.05), or radiological cancer diagnosis (OR 2.02, 95% CI 1.13-3.60). Thirty-day mortality rates following ERCP and PTBD were 21.4% and 21.4%, respectively, in unresectable cancer and 6% and 6.3%, respectively, in potentially resectable cancer. Increased 30-day mortality in patients with unresectable disease was associated with a performance status of 2 or more (HR 3.14 (1.65-5.97)). Thirty-day mortality was significantly higher in patients with unresectable cancer if a multidisciplinary team meeting had not reviewed and advised drainage prior to the procedure 50% vs 20.4% ( <i>P</i> = 0.028).</p><p><strong>Conclusions: </strong>Careful multidisciplinary consideration of risks and potential benefits should be undertaken prior to attempting malignant biliary drainage due to the high risk of complications and early mortality.</p>\",\"PeriodicalId\":11671,\"journal\":{\"name\":\"Endoscopy International Open\",\"volume\":\"13 \",\"pages\":\"a25586754\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-07-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303028/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Endoscopy International Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2558-6754\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endoscopy International Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2558-6754","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景和研究目的:国家数据显示,胆道引流治疗恶性梗阻的并发症发生率高,早期死亡率高。这项研究调查了与不良结果相关的因素。患者和方法:RICOCHET是一项针对2018年4月至8月期间胰腺癌或恶性胆道梗阻患者的全国性前瞻性审计。本分析回顾了胆道引流术后7天内并发症和30天死亡率及相关因素。结果:773例患者尝试胆道引流,78.7%首次成功;但如果失败,只有37%的后续尝试成功。11%的内窥镜逆行胆管造影(ercp)(包括胰腺炎,5%)和12%的经皮经肝胆道引流(ptbd)(包括胆管炎,8%)发生并发症。并发症与潜在可切除的癌症相关(优势比[OR] 1.93, 95%可信区间[CI] 1.23-3.03);一次以上胆道引流尝试(OR 1.69, 95% CI 1.04-2.74);胆管癌(OR 2.20, 95% CI 1.20-4.05)或放射学癌症诊断(OR 2.02, 95% CI 1.13-3.60)。在不可切除的癌症中,ERCP和PTBD的30天死亡率分别为21.4%和21.4%,而在可能可切除的癌症中,ERCP和PTBD的30天死亡率分别为6%和6.3%。不可切除疾病患者的30天死亡率增加与2或以上的表现状态相关(HR 3.14(1.65-5.97))。对于无法切除的癌症患者,如果术前未召开多学科小组会议并建议引流,则30天死亡率明显高于50%和20.4% (P = 0.028)。结论:由于并发症和早期死亡的高风险,在尝试恶性胆道引流之前,应仔细考虑风险和潜在的益处。
Outcomes and complications of biliary drainage for malignant biliary obstruction: National prospective study.
Background and study aims: National data suggest that biliary drainage for malignant obstruction is associated with high complication rates and early mortality. This study examined factors associated with poor outcomes.
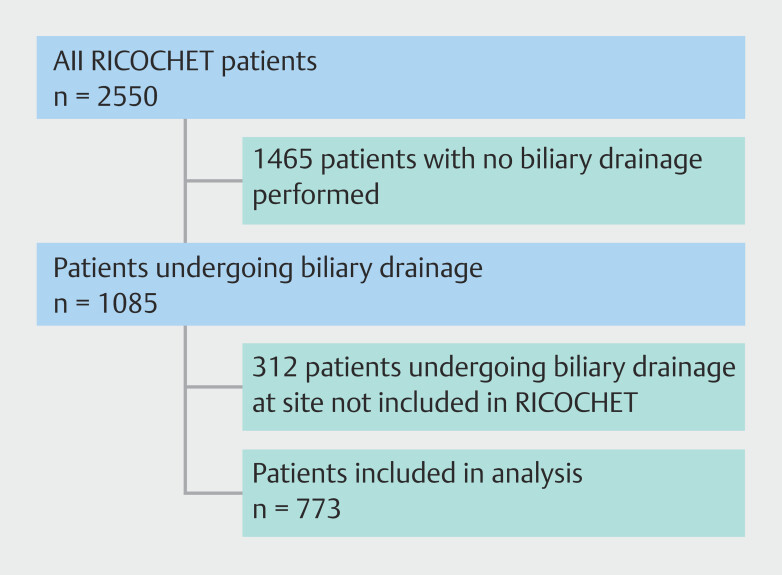
Patients and methods: RICOCHET was a national, prospective audit of patients with pancreatic cancer or malignant biliary obstruction between April and August 2018. This analysis reviewed outcomes including complications within 7 days and 30-day mortality following biliary drainage and associated factors.
Results: Biliary drainage was attempted in 773 patients, of which, 78.7% were successful at first attempt; but if unsuccessful, only 37% of subsequent attempts succeeded. Complications occurred following 11% of endoscopic retrograde cholangiopancreatographies (ERCPs) (including pancreatitis, 5%) and 12% of percutaneous transhepatic biliary drainages (PTBDs) (including cholangitis, 8%). Complications were associated with: potentially resectable cancer (odds ratio [OR] 1.93, 95% confidence interval [CI] 1.23-3.03); more than one biliary drainage attempt (OR 1.69, 95% CI 1.04-2.74); cholangiocarcinoma (OR 2.20, 95% CI 1.20-4.05), or radiological cancer diagnosis (OR 2.02, 95% CI 1.13-3.60). Thirty-day mortality rates following ERCP and PTBD were 21.4% and 21.4%, respectively, in unresectable cancer and 6% and 6.3%, respectively, in potentially resectable cancer. Increased 30-day mortality in patients with unresectable disease was associated with a performance status of 2 or more (HR 3.14 (1.65-5.97)). Thirty-day mortality was significantly higher in patients with unresectable cancer if a multidisciplinary team meeting had not reviewed and advised drainage prior to the procedure 50% vs 20.4% ( P = 0.028).
Conclusions: Careful multidisciplinary consideration of risks and potential benefits should be undertaken prior to attempting malignant biliary drainage due to the high risk of complications and early mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


