Andrew Achaiah, Emily Fraser, Peter Saunders, Rachel Hoyles, Rachel Benamore, Ling-Pei Ho
{"title":"一项单中心队列研究的结果表明,血液白细胞、强制肺活量和定量CT的综合测量可高度预测IPF患者的死亡率。","authors":"Andrew Achaiah, Emily Fraser, Peter Saunders, Rachel Hoyles, Rachel Benamore, Ling-Pei Ho","doi":"10.1186/s12890-025-03825-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Idiopathic pulmonary fibrosis (IPF) is a progressive fibrotic condition. Serial FVC monitoring is most commonly used to assess progression of disease but FVC does not always reflect regional CT change in IPF. Recently there has been growing interest in quantitative CT (qCT) assessment of IPF. In this study, we compared different physiological and qCT measurements of disease progression in predicting mortality in IPF.</p><p><strong>Aims: </strong>We question if a composite measure of disease progression using qCT and FVC is more predictive of mortality than individual measurements, and if addition of blood leukocyte levels further enhance predictive ability of these measurements of disease progression.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of an IPF cohort (n = 71). Annualised change (∆) in CT-measured lung volume (CTvol) and total lung fibrosis score (TLF) were calculated (using the computer software CALIPER) together with annualised change in FVC and blood leukocyte levels within 4 months of first CT. These were modelled against mortality using multivariate Cox regression. Concordance indexes (C-statistic) of different Cox regression models were used to determine the most predictive and discriminative combination for mortality.</p><p><strong>Results: </strong>65 cases (91.5%) were male. Median (IQR) age 73.6 years (68.4-79.3). Death was reported in 24 cases (33.8%). The median annualised change in (∆)FVC was - 4.4% (-9.6-0.0), ∆TLF; + 2.9% (0.2-7.0), and ∆CTvol; -4.3% (0.0-10.9). Combined measurements of disease progression (∆CTvol, ∆FVC and ∆TLF%) out-performed single-variable measurements in predicting all-cause mortality in IPF. The composite variable of [ΔFVC >10%, ΔCTvol >10% or ΔTLF% >10%] was most predictive of mortality [HR 7.14 (2.45-20.79), p <0.001]. Inclusion of blood leukocytes improved C-statistic scores for each multivariate model.</p><p><strong>Conclusion: </strong>Composite end points of ∆CTvol, ∆FVC and ∆TLF% were more predictive of mortality than single-variable measurements in this cohort. Inclusion of blood leukocytes into risk stratification models further improved mortality prediction for all measures of disease progression.</p>","PeriodicalId":9148,"journal":{"name":"BMC Pulmonary Medicine","volume":"25 1","pages":"358"},"PeriodicalIF":2.8000,"publicationDate":"2025-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12302753/pdf/","citationCount":"0","resultStr":"{\"title\":\"A combined measure of blood leukocytes, forced vital capacity and quantitative CT is highly predictive of mortality in IPF: results of a single-centre cohort study.\",\"authors\":\"Andrew Achaiah, Emily Fraser, Peter Saunders, Rachel Hoyles, Rachel Benamore, Ling-Pei Ho\",\"doi\":\"10.1186/s12890-025-03825-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Idiopathic pulmonary fibrosis (IPF) is a progressive fibrotic condition. Serial FVC monitoring is most commonly used to assess progression of disease but FVC does not always reflect regional CT change in IPF. Recently there has been growing interest in quantitative CT (qCT) assessment of IPF. In this study, we compared different physiological and qCT measurements of disease progression in predicting mortality in IPF.</p><p><strong>Aims: </strong>We question if a composite measure of disease progression using qCT and FVC is more predictive of mortality than individual measurements, and if addition of blood leukocyte levels further enhance predictive ability of these measurements of disease progression.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of an IPF cohort (n = 71). Annualised change (∆) in CT-measured lung volume (CTvol) and total lung fibrosis score (TLF) were calculated (using the computer software CALIPER) together with annualised change in FVC and blood leukocyte levels within 4 months of first CT. These were modelled against mortality using multivariate Cox regression. Concordance indexes (C-statistic) of different Cox regression models were used to determine the most predictive and discriminative combination for mortality.</p><p><strong>Results: </strong>65 cases (91.5%) were male. Median (IQR) age 73.6 years (68.4-79.3). Death was reported in 24 cases (33.8%). The median annualised change in (∆)FVC was - 4.4% (-9.6-0.0), ∆TLF; + 2.9% (0.2-7.0), and ∆CTvol; -4.3% (0.0-10.9). Combined measurements of disease progression (∆CTvol, ∆FVC and ∆TLF%) out-performed single-variable measurements in predicting all-cause mortality in IPF. The composite variable of [ΔFVC >10%, ΔCTvol >10% or ΔTLF% >10%] was most predictive of mortality [HR 7.14 (2.45-20.79), p <0.001]. Inclusion of blood leukocytes improved C-statistic scores for each multivariate model.</p><p><strong>Conclusion: </strong>Composite end points of ∆CTvol, ∆FVC and ∆TLF% were more predictive of mortality than single-variable measurements in this cohort. Inclusion of blood leukocytes into risk stratification models further improved mortality prediction for all measures of disease progression.</p>\",\"PeriodicalId\":9148,\"journal\":{\"name\":\"BMC Pulmonary Medicine\",\"volume\":\"25 1\",\"pages\":\"358\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-07-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12302753/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Pulmonary Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12890-025-03825-4\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Pulmonary Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12890-025-03825-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
A combined measure of blood leukocytes, forced vital capacity and quantitative CT is highly predictive of mortality in IPF: results of a single-centre cohort study.
Background: Idiopathic pulmonary fibrosis (IPF) is a progressive fibrotic condition. Serial FVC monitoring is most commonly used to assess progression of disease but FVC does not always reflect regional CT change in IPF. Recently there has been growing interest in quantitative CT (qCT) assessment of IPF. In this study, we compared different physiological and qCT measurements of disease progression in predicting mortality in IPF.
Aims: We question if a composite measure of disease progression using qCT and FVC is more predictive of mortality than individual measurements, and if addition of blood leukocyte levels further enhance predictive ability of these measurements of disease progression.
Methods: We conducted a retrospective analysis of an IPF cohort (n = 71). Annualised change (∆) in CT-measured lung volume (CTvol) and total lung fibrosis score (TLF) were calculated (using the computer software CALIPER) together with annualised change in FVC and blood leukocyte levels within 4 months of first CT. These were modelled against mortality using multivariate Cox regression. Concordance indexes (C-statistic) of different Cox regression models were used to determine the most predictive and discriminative combination for mortality.
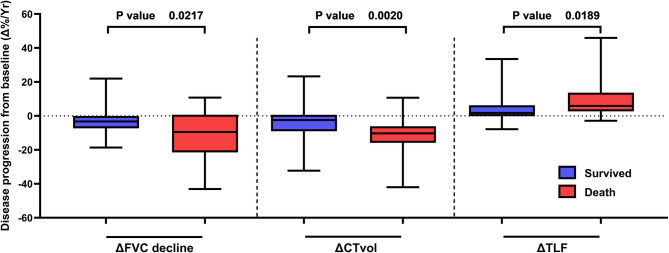
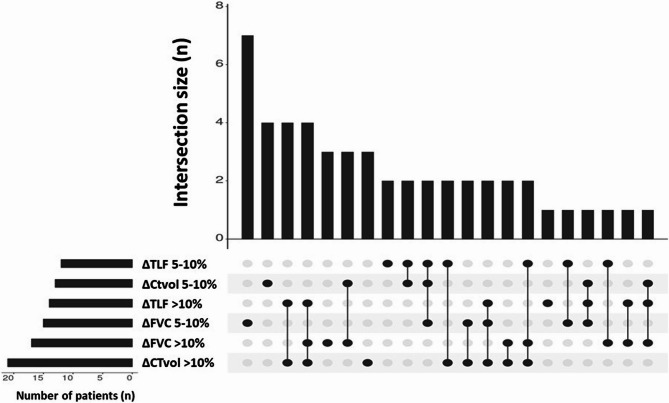
Results: 65 cases (91.5%) were male. Median (IQR) age 73.6 years (68.4-79.3). Death was reported in 24 cases (33.8%). The median annualised change in (∆)FVC was - 4.4% (-9.6-0.0), ∆TLF; + 2.9% (0.2-7.0), and ∆CTvol; -4.3% (0.0-10.9). Combined measurements of disease progression (∆CTvol, ∆FVC and ∆TLF%) out-performed single-variable measurements in predicting all-cause mortality in IPF. The composite variable of [ΔFVC >10%, ΔCTvol >10% or ΔTLF% >10%] was most predictive of mortality [HR 7.14 (2.45-20.79), p <0.001]. Inclusion of blood leukocytes improved C-statistic scores for each multivariate model.
Conclusion: Composite end points of ∆CTvol, ∆FVC and ∆TLF% were more predictive of mortality than single-variable measurements in this cohort. Inclusion of blood leukocytes into risk stratification models further improved mortality prediction for all measures of disease progression.
期刊介绍:
BMC Pulmonary Medicine is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of pulmonary and associated disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


