Justin Bradley, Mollie Rumble, Jennifer Wong, Ming Yii, Michelle R Kaminski
{"title":"评估活动性Charcot神经骨关节病患者皮肤温度的全接触铸造(TCC)去除后达到温度稳定的最佳时间。","authors":"Justin Bradley, Mollie Rumble, Jennifer Wong, Ming Yii, Michelle R Kaminski","doi":"10.1002/jfa2.70059","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Dermal temperature differentials between limbs are used to monitor disease progression and support safe withdrawal of immobilisation in Charcot neuro-osteoarthropathy (CNO). Despite the wide clinical use of dermal thermometry, there is a lack of evidence on the optimal temperature stabilisation period after removal of immobilisation devices, such as total contact casts (TCCs). This study aimed to investigate the optimal time period to achieve temperature stabilisation post removal of TCC for assessing dermal temperatures in active CNO.</p><p><strong>Methods: </strong>Over a 2-year period, this within-subjects repeated measures study recruited 12 adults with active CNO treated with TCC from a metropolitan high-risk foot service in Melbourne, Australia. Participants were excluded if they had bilateral CNO, an active foot ulcer, an inflammatory foot condition (e.g., gout), peripheral artery disease or major lower limb amputation. In a temperature-controlled room, dermal temperatures were recorded using an infrared thermometer after removal of TCC and contralateral footwear. Temperatures were recorded at 10-min intervals from baseline to 90 min at 10 anatomical locations on each foot. Paired samples t-tests or Wilcoxon signed-rank tests explored temperature stabilisation at each anatomical site across the 10 time points.</p><p><strong>Results: </strong>Mean age was 55.1 (SD, 8.9) years, 75.0% were male and 83.3% had type 2 diabetes. All participants had peripheral neuropathy and a large proportion had history of foot ulceration (75.0%). The average duration of CNO was 2.9 (SD, 1.7) months, with most classified as stage 1 (91.7%), affecting the tarsometatarsal joints (58.3%) and midtarsal joints (83.3%). Overall, dermal temperatures had stabilised by 40 min for the Charcot (casted) foot and contralateral (non-casted) foot.</p><p><strong>Conclusions: </strong>This is the first study to explore the optimal time period to achieve temperature stabilisation when assessing dermal temperatures in active CNO. Forty minutes appears to be an appropriate resting time to reach thermal equilibrium. Although this approach may improve the accuracy of dermal thermometry, the time period may not always be feasible in clinical practice.</p>","PeriodicalId":49164,"journal":{"name":"Journal of Foot and Ankle Research","volume":"18 3","pages":"e70059"},"PeriodicalIF":2.2000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12461229/pdf/","citationCount":"0","resultStr":"{\"title\":\"Optimal Time Period to Achieve Temperature Stabilisation After Total Contact Cast (TCC) Removal for Assessing Dermal Temperatures in Active Charcot Neuro-Osteoarthropathy.\",\"authors\":\"Justin Bradley, Mollie Rumble, Jennifer Wong, Ming Yii, Michelle R Kaminski\",\"doi\":\"10.1002/jfa2.70059\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Dermal temperature differentials between limbs are used to monitor disease progression and support safe withdrawal of immobilisation in Charcot neuro-osteoarthropathy (CNO). Despite the wide clinical use of dermal thermometry, there is a lack of evidence on the optimal temperature stabilisation period after removal of immobilisation devices, such as total contact casts (TCCs). This study aimed to investigate the optimal time period to achieve temperature stabilisation post removal of TCC for assessing dermal temperatures in active CNO.</p><p><strong>Methods: </strong>Over a 2-year period, this within-subjects repeated measures study recruited 12 adults with active CNO treated with TCC from a metropolitan high-risk foot service in Melbourne, Australia. Participants were excluded if they had bilateral CNO, an active foot ulcer, an inflammatory foot condition (e.g., gout), peripheral artery disease or major lower limb amputation. In a temperature-controlled room, dermal temperatures were recorded using an infrared thermometer after removal of TCC and contralateral footwear. Temperatures were recorded at 10-min intervals from baseline to 90 min at 10 anatomical locations on each foot. Paired samples t-tests or Wilcoxon signed-rank tests explored temperature stabilisation at each anatomical site across the 10 time points.</p><p><strong>Results: </strong>Mean age was 55.1 (SD, 8.9) years, 75.0% were male and 83.3% had type 2 diabetes. All participants had peripheral neuropathy and a large proportion had history of foot ulceration (75.0%). The average duration of CNO was 2.9 (SD, 1.7) months, with most classified as stage 1 (91.7%), affecting the tarsometatarsal joints (58.3%) and midtarsal joints (83.3%). Overall, dermal temperatures had stabilised by 40 min for the Charcot (casted) foot and contralateral (non-casted) foot.</p><p><strong>Conclusions: </strong>This is the first study to explore the optimal time period to achieve temperature stabilisation when assessing dermal temperatures in active CNO. Forty minutes appears to be an appropriate resting time to reach thermal equilibrium. Although this approach may improve the accuracy of dermal thermometry, the time period may not always be feasible in clinical practice.</p>\",\"PeriodicalId\":49164,\"journal\":{\"name\":\"Journal of Foot and Ankle Research\",\"volume\":\"18 3\",\"pages\":\"e70059\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12461229/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Foot and Ankle Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/jfa2.70059\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Foot and Ankle Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/jfa2.70059","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Optimal Time Period to Achieve Temperature Stabilisation After Total Contact Cast (TCC) Removal for Assessing Dermal Temperatures in Active Charcot Neuro-Osteoarthropathy.
Background: Dermal temperature differentials between limbs are used to monitor disease progression and support safe withdrawal of immobilisation in Charcot neuro-osteoarthropathy (CNO). Despite the wide clinical use of dermal thermometry, there is a lack of evidence on the optimal temperature stabilisation period after removal of immobilisation devices, such as total contact casts (TCCs). This study aimed to investigate the optimal time period to achieve temperature stabilisation post removal of TCC for assessing dermal temperatures in active CNO.
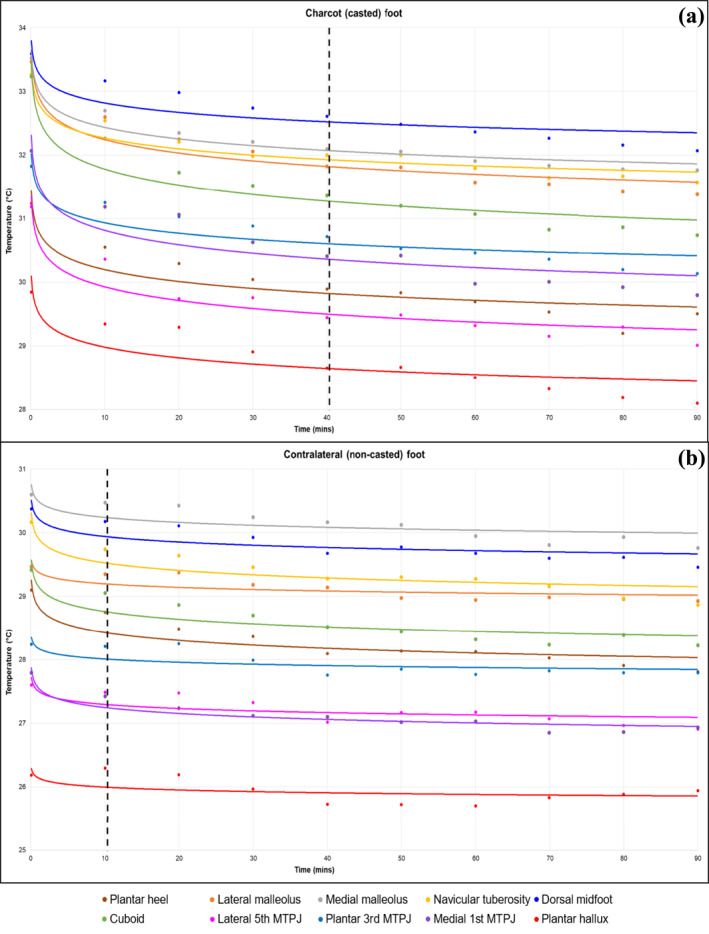
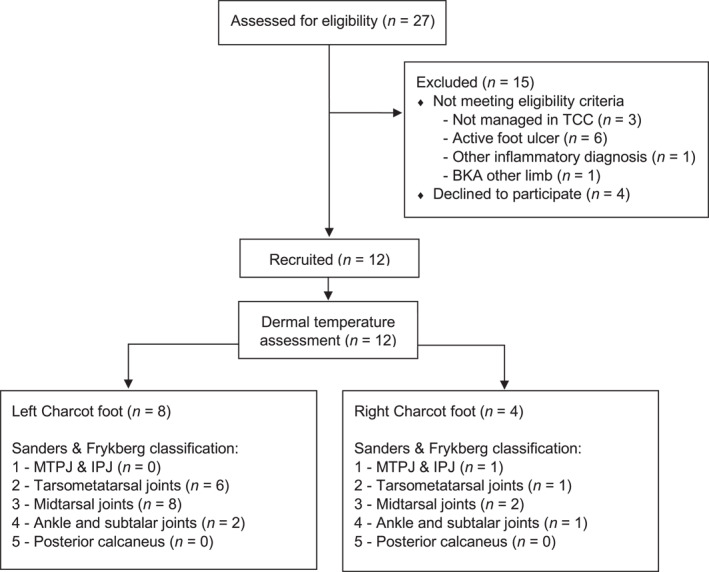
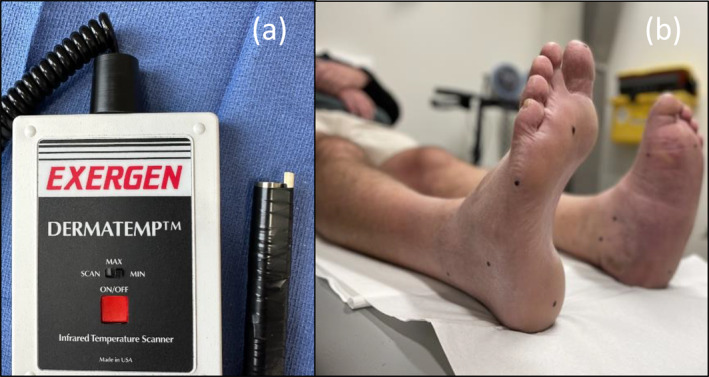
Methods: Over a 2-year period, this within-subjects repeated measures study recruited 12 adults with active CNO treated with TCC from a metropolitan high-risk foot service in Melbourne, Australia. Participants were excluded if they had bilateral CNO, an active foot ulcer, an inflammatory foot condition (e.g., gout), peripheral artery disease or major lower limb amputation. In a temperature-controlled room, dermal temperatures were recorded using an infrared thermometer after removal of TCC and contralateral footwear. Temperatures were recorded at 10-min intervals from baseline to 90 min at 10 anatomical locations on each foot. Paired samples t-tests or Wilcoxon signed-rank tests explored temperature stabilisation at each anatomical site across the 10 time points.
Results: Mean age was 55.1 (SD, 8.9) years, 75.0% were male and 83.3% had type 2 diabetes. All participants had peripheral neuropathy and a large proportion had history of foot ulceration (75.0%). The average duration of CNO was 2.9 (SD, 1.7) months, with most classified as stage 1 (91.7%), affecting the tarsometatarsal joints (58.3%) and midtarsal joints (83.3%). Overall, dermal temperatures had stabilised by 40 min for the Charcot (casted) foot and contralateral (non-casted) foot.
Conclusions: This is the first study to explore the optimal time period to achieve temperature stabilisation when assessing dermal temperatures in active CNO. Forty minutes appears to be an appropriate resting time to reach thermal equilibrium. Although this approach may improve the accuracy of dermal thermometry, the time period may not always be feasible in clinical practice.
期刊介绍:
Journal of Foot and Ankle Research, the official journal of the Australian Podiatry Association and The College of Podiatry (UK), is an open access journal that encompasses all aspects of policy, organisation, delivery and clinical practice related to the assessment, diagnosis, prevention and management of foot and ankle disorders.
Journal of Foot and Ankle Research covers a wide range of clinical subject areas, including diabetology, paediatrics, sports medicine, gerontology and geriatrics, foot surgery, physical therapy, dermatology, wound management, radiology, biomechanics and bioengineering, orthotics and prosthetics, as well the broad areas of epidemiology, policy, organisation and delivery of services related to foot and ankle care.
The journal encourages submissions from all health professionals who manage lower limb conditions, including podiatrists, nurses, physical therapists and physiotherapists, orthopaedists, manual therapists, medical specialists and general medical practitioners, as well as health service researchers concerned with foot and ankle care.
The Australian Podiatry Association and the College of Podiatry (UK) have reserve funds to cover the article-processing charge for manuscripts submitted by its members. Society members can email the appropriate contact at Australian Podiatry Association or The College of Podiatry to obtain the corresponding code to enter on submission.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


