Xiaojie Wang, Jingyu Zou, Yanwu Sun, Zhifang Zheng, Yongqin Tang, Shenghui Huang, Ying Huang, Pan Chi
{"title":"基于淋巴结阳性状态的直肠癌新辅助CRT后淋巴结计数对肿瘤预后的反作用:一项大量中国中心经验。","authors":"Xiaojie Wang, Jingyu Zou, Yanwu Sun, Zhifang Zheng, Yongqin Tang, Shenghui Huang, Ying Huang, Pan Chi","doi":"10.1007/s00384-025-04913-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neoadjuvant chemoradiation therapy (CRT) followed by total mesorectal excision (TME) is the standard of care for locally advanced rectal cancer (LARC). Current guidelines recommend dissecting at least 12 lymph nodes (LNs). However, the impact of LN count post-CRT on survival outcomes remains controversial. This study aimed to evaluate the relationship between LN count and oncologic outcomes in LARC patients treated with neoadjuvant CRT followed by surgery.</p><p><strong>Methods: </strong>This retrospective analysis was conducted on 1483 patients with cT3-4N + LARC who underwent neoadjuvant CRT and curative resection. Univariate and multivariate analyses were performed to identify factors associated with achieving 12 or more LNs. Restricted cubic spline (RCS) and Cox proportional hazards models were used to assess the relationship between LN count and oncologic outcomes, including disease-free survival (DFS) and overall survival (OS). Exploratory subgroup analyses stratified patients by ypN positivity status.</p><p><strong>Results: </strong>The mean number of LNs retrieved was 12.9 ± 6.8, with 55.7% of patients having 12 or more LNs examined. Laparoscopic surgery, tumor location (mid rectum), younger age, and lymph node status (pN2) were independent factors associated with achieving 12 or more LNs. RCS analysis revealed an inverse relationship between LN count and tumor response to CRT, but no association with OS and DFS in the overall cohort. ypN-negative patients tended to have a higher rate of liver metastases with an increased LN count (P = 0.010). However, in ypN-positive patients, a higher LN count was associated with improved DFS (P = 0.007) and a lower likelihood of lung metastases (P = 0.001). Using X-tile software, a cutoff value of 10 LNs was identified as optimal for DFS in stage 3 rectal cancer patients. Patients with 11 or more LNs examined had significantly better 5-year DFS (66.7% vs. 55.8%, P = 0.035) compared to those with fewer than 11 LNs.</p><p><strong>Conclusion: </strong>Our study challenges the guideline of examining at least 12 LNs during rectal cancer surgery after CRT, as we observed an inverse relationship between LN count and tumor response to CRT. The inverse effects of LN count on oncological outcomes across various stages of LN positivity highlight the need for individualized treatment strategies based on lymph node positivity status. For ypN-negative patients, understanding that an increased LN count is associated with a higher risk of liver metastases can help identify high-risk stage 0-2 patients who may benefit from adjuvant therapy. For ypN-positive (stage 3) patients, achieving at least 11 LNs is necessary to ensure better oncological outcomes.</p>","PeriodicalId":13789,"journal":{"name":"International Journal of Colorectal Disease","volume":"40 1","pages":"163"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12296959/pdf/","citationCount":"0","resultStr":"{\"title\":\"Inverse effects of lymph node count on oncological outcomes in rectal cancer based on lymph node positivity status post-neoadjuvant CRT: a large-volume Chinese center experience.\",\"authors\":\"Xiaojie Wang, Jingyu Zou, Yanwu Sun, Zhifang Zheng, Yongqin Tang, Shenghui Huang, Ying Huang, Pan Chi\",\"doi\":\"10.1007/s00384-025-04913-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Neoadjuvant chemoradiation therapy (CRT) followed by total mesorectal excision (TME) is the standard of care for locally advanced rectal cancer (LARC). Current guidelines recommend dissecting at least 12 lymph nodes (LNs). However, the impact of LN count post-CRT on survival outcomes remains controversial. This study aimed to evaluate the relationship between LN count and oncologic outcomes in LARC patients treated with neoadjuvant CRT followed by surgery.</p><p><strong>Methods: </strong>This retrospective analysis was conducted on 1483 patients with cT3-4N + LARC who underwent neoadjuvant CRT and curative resection. Univariate and multivariate analyses were performed to identify factors associated with achieving 12 or more LNs. Restricted cubic spline (RCS) and Cox proportional hazards models were used to assess the relationship between LN count and oncologic outcomes, including disease-free survival (DFS) and overall survival (OS). Exploratory subgroup analyses stratified patients by ypN positivity status.</p><p><strong>Results: </strong>The mean number of LNs retrieved was 12.9 ± 6.8, with 55.7% of patients having 12 or more LNs examined. Laparoscopic surgery, tumor location (mid rectum), younger age, and lymph node status (pN2) were independent factors associated with achieving 12 or more LNs. RCS analysis revealed an inverse relationship between LN count and tumor response to CRT, but no association with OS and DFS in the overall cohort. ypN-negative patients tended to have a higher rate of liver metastases with an increased LN count (P = 0.010). However, in ypN-positive patients, a higher LN count was associated with improved DFS (P = 0.007) and a lower likelihood of lung metastases (P = 0.001). Using X-tile software, a cutoff value of 10 LNs was identified as optimal for DFS in stage 3 rectal cancer patients. Patients with 11 or more LNs examined had significantly better 5-year DFS (66.7% vs. 55.8%, P = 0.035) compared to those with fewer than 11 LNs.</p><p><strong>Conclusion: </strong>Our study challenges the guideline of examining at least 12 LNs during rectal cancer surgery after CRT, as we observed an inverse relationship between LN count and tumor response to CRT. The inverse effects of LN count on oncological outcomes across various stages of LN positivity highlight the need for individualized treatment strategies based on lymph node positivity status. For ypN-negative patients, understanding that an increased LN count is associated with a higher risk of liver metastases can help identify high-risk stage 0-2 patients who may benefit from adjuvant therapy. For ypN-positive (stage 3) patients, achieving at least 11 LNs is necessary to ensure better oncological outcomes.</p>\",\"PeriodicalId\":13789,\"journal\":{\"name\":\"International Journal of Colorectal Disease\",\"volume\":\"40 1\",\"pages\":\"163\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-07-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12296959/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Colorectal Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00384-025-04913-x\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Colorectal Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00384-025-04913-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:新辅助放化疗(CRT)后全肠系膜切除(TME)是局部晚期直肠癌(LARC)的标准治疗方法。目前的指南建议至少清扫12个淋巴结(LNs)。然而,crt后LN计数对生存结果的影响仍然存在争议。本研究旨在评估LARC患者接受新辅助CRT治疗后手术后LN计数与肿瘤预后之间的关系。方法:回顾性分析1483例cT3-4N + LARC行新辅助CRT和根治性切除的病例。进行单因素和多因素分析以确定与达到12个或更多LNs相关的因素。使用限制性三次样条(RCS)和Cox比例风险模型来评估LN计数与肿瘤预后(包括无病生存期(DFS)和总生存期(OS))之间的关系。探索性亚组分析以ypN阳性状态对患者进行分层。结果:平均取到的LNs数为12.9±6.8个,其中55.7%的患者检查了12个或以上的LNs。腹腔镜手术、肿瘤位置(直肠中部)、年龄较小和淋巴结状态(pN2)是获得12个或更多LNs的独立因素。RCS分析显示LN计数与肿瘤对CRT的反应呈负相关,但与总体队列的OS和DFS无关联。随着LN计数的增加,ypn阴性患者的肝转移率更高(P = 0.010)。然而,在ypn阳性患者中,较高的LN计数与改善的DFS (P = 0.007)和较低的肺转移可能性(P = 0.001)相关。使用X-tile软件,确定10 LNs的截断值为3期直肠癌患者DFS的最佳值。与小于11个LNs的患者相比,检查了11个或更多LNs的患者的5年DFS明显更好(66.7% vs. 55.8%, P = 0.035)。结论:我们的研究挑战了在直肠癌CRT术后检查至少12个LN的指南,因为我们观察到LN计数与肿瘤对CRT的反应呈反比关系。LN计数在LN阳性的不同阶段对肿瘤结果的反作用强调了基于淋巴结阳性状态的个性化治疗策略的必要性。对于ypn阴性患者,了解LN计数增加与肝转移风险增加相关可以帮助识别可能从辅助治疗中获益的高危0-2期患者。对于ypn阳性(3期)患者,达到至少11ln是确保更好的肿瘤预后所必需的。
Inverse effects of lymph node count on oncological outcomes in rectal cancer based on lymph node positivity status post-neoadjuvant CRT: a large-volume Chinese center experience.
Background: Neoadjuvant chemoradiation therapy (CRT) followed by total mesorectal excision (TME) is the standard of care for locally advanced rectal cancer (LARC). Current guidelines recommend dissecting at least 12 lymph nodes (LNs). However, the impact of LN count post-CRT on survival outcomes remains controversial. This study aimed to evaluate the relationship between LN count and oncologic outcomes in LARC patients treated with neoadjuvant CRT followed by surgery.
Methods: This retrospective analysis was conducted on 1483 patients with cT3-4N + LARC who underwent neoadjuvant CRT and curative resection. Univariate and multivariate analyses were performed to identify factors associated with achieving 12 or more LNs. Restricted cubic spline (RCS) and Cox proportional hazards models were used to assess the relationship between LN count and oncologic outcomes, including disease-free survival (DFS) and overall survival (OS). Exploratory subgroup analyses stratified patients by ypN positivity status.
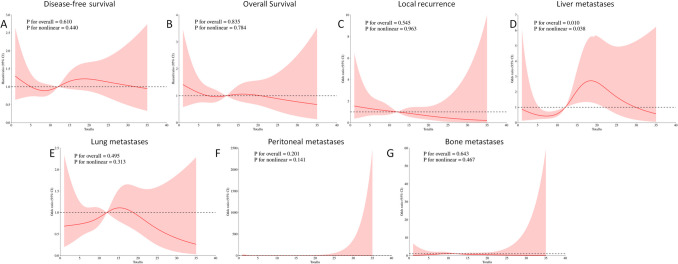
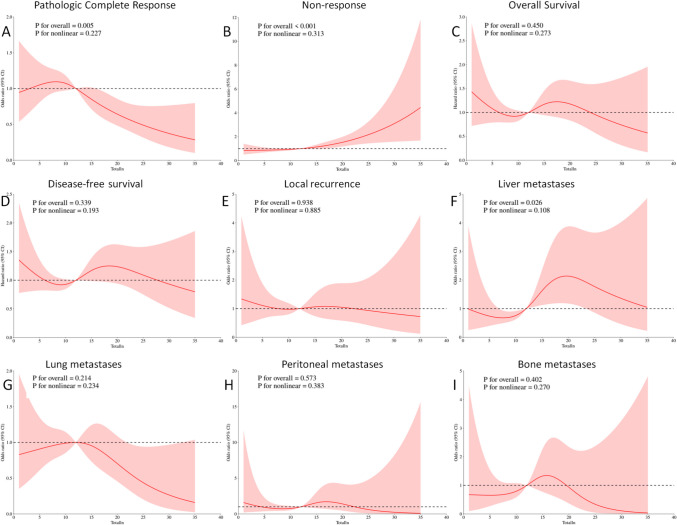
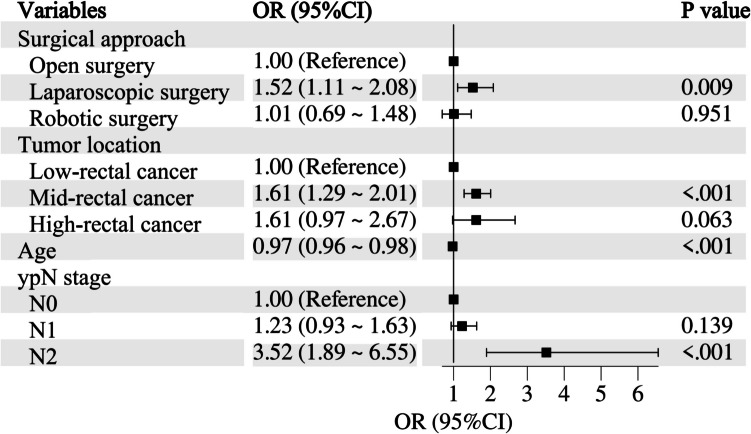
Results: The mean number of LNs retrieved was 12.9 ± 6.8, with 55.7% of patients having 12 or more LNs examined. Laparoscopic surgery, tumor location (mid rectum), younger age, and lymph node status (pN2) were independent factors associated with achieving 12 or more LNs. RCS analysis revealed an inverse relationship between LN count and tumor response to CRT, but no association with OS and DFS in the overall cohort. ypN-negative patients tended to have a higher rate of liver metastases with an increased LN count (P = 0.010). However, in ypN-positive patients, a higher LN count was associated with improved DFS (P = 0.007) and a lower likelihood of lung metastases (P = 0.001). Using X-tile software, a cutoff value of 10 LNs was identified as optimal for DFS in stage 3 rectal cancer patients. Patients with 11 or more LNs examined had significantly better 5-year DFS (66.7% vs. 55.8%, P = 0.035) compared to those with fewer than 11 LNs.
Conclusion: Our study challenges the guideline of examining at least 12 LNs during rectal cancer surgery after CRT, as we observed an inverse relationship between LN count and tumor response to CRT. The inverse effects of LN count on oncological outcomes across various stages of LN positivity highlight the need for individualized treatment strategies based on lymph node positivity status. For ypN-negative patients, understanding that an increased LN count is associated with a higher risk of liver metastases can help identify high-risk stage 0-2 patients who may benefit from adjuvant therapy. For ypN-positive (stage 3) patients, achieving at least 11 LNs is necessary to ensure better oncological outcomes.
期刊介绍:
The International Journal of Colorectal Disease, Clinical and Molecular Gastroenterology and Surgery aims to publish novel and state-of-the-art papers which deal with the physiology and pathophysiology of diseases involving the entire gastrointestinal tract. In addition to original research articles, the following categories will be included: reviews (usually commissioned but may also be submitted), case reports, letters to the editor, and protocols on clinical studies.
The journal offers its readers an interdisciplinary forum for clinical science and molecular research related to gastrointestinal disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


