有和没有复苏的休克性心脏骤停患者的心源性休克的比较特征和结果:来自FRENSHOCK多中心前瞻性登记的见解
IF 2.4
Q3 CRITICAL CARE MEDICINE
引用次数: 0
摘要
目的心源性休克(CS)伴和未伴心脏骤停(CA)的差异在很大程度上仍未被研究。我们假设,与之前没有发生过CA的患者相比,经历过震荡性CA后发生CS的患者可能有更差的结果。方法frenshock是2016年在法国重症监护病房进行的一项前瞻性多中心观察性注册研究,其中包括各种病因的CS。在CA复苏后入院的患者如果符合先前定义的CS标准则纳入。医疗干预时的非电击性心律被视为排除标准,未记录在登记册中。结果771例入组患者(平均年龄65.7±14.9岁;71.5%(男性),79例(10.2%)在纳入前出现复苏的休克性心脏骤停。休克性CA患者有更多的呼吸支持(78.5% vs 33.2%, p <;0.001),更多的机械循环支持(35.4%比16.5%,p <;0.001),更多的冠状动脉造影(76%比48.8%,p <;0.001),发现更多的单结节性病变(39% vs. 16.9%, p <;0.001)。两组间30天和1年生存率相似。在30天的幸存者中,与没有事先复苏CA的CS相比,最初发生休克性CA的CS表现出显著提高的长期生存率。结论:在一组来自各种病因的心源性休克患者中,大约10%的患者在心脏骤停后经历了事先复苏。我们的研究结果表明,与其他原因的心源性休克相比,选择性心脏骤停伴震荡性心律导致的心源性休克并不一定具有更差的预后。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Comparative features and outcomes of cardiogenic shock in patients with and without prior resuscitated shockable cardiac arrest: Insight from the FRENSHOCK multicenter prospective registry
Aim
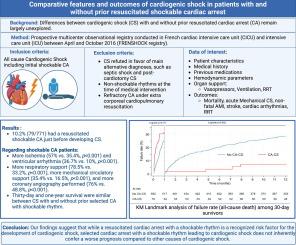
Differences between cardiogenic shock (CS) with and without prior resuscitated cardiac arrest (CA) remain largely unexplored. We hypothesized that patients who experience shockable CA followed by CS are likely to have worse outcomes compared to CS without prior CA.
Methods
FRENSHOCK is a prospective multicenter observational registry conducted in French critical care units in 2016, which included CS from various etiologies. Patients admitted after resuscitation of a CA were included if they fulfilled previously defined CS criteria. Non-shockable rhythms at the time of medical intervention were considered exclusion criteria and were not recorded in the registry.
Results
Among the 771 enrolled patients (mean age 65.7 ± 14.9 years; 71.5 % male), 79 (10.2 %) had a resuscitated shockable cardiac arrest just before inclusion. Shockable CA patients had more respiratory support (78.5 % vs. 33.2 %, p < 0.001), more mechanical circulatory support (35.4 % vs. 16.5 %, p < 0.001), more coronary angiography performed (76 % vs. 48.8 %, p < 0.001), finding more mono-troncular lesions (39 % vs. 16.9 %, p < 0.001). Thirty-day and one-year survival were similar between groups. Among 30-day survivors, CS with an initial shockable CA exhibited significantly improved long-term survival compared to CS without prior resuscitated CA.
Conclusion
In a cohort of patients with cardiogenic shock from various etiologies, approximately 10% had experienced prior resuscitation following a cardiac arrest with shockable rhythms. Our findings suggest that selected cardiac arrest with a shockable rhythm leading to cardiogenic shock does not inherently confer a worse prognosis compared to other causes of cardiogenic shock.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

Resuscitation plus
Critical Care and Intensive Care Medicine, Emergency Medicine
CiteScore
3.00
自引率
0.00%
发文量
0
审稿时长
52 days
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


