Roland I Stephen, Jimmy A Reyes, Jacob A Dunga, Sati K Awang, Kefas P Zawaya
{"title":"在直接抗病毒药物的持续病毒学应答后,终末期丙型肝炎相关晚期肝硬化患者的异常生存期为6.5年——来自低资源环境的一例报告。","authors":"Roland I Stephen, Jimmy A Reyes, Jacob A Dunga, Sati K Awang, Kefas P Zawaya","doi":"10.71480/nmj.v66i2.661","DOIUrl":null,"url":null,"abstract":"<p><p>Advanced chronic liver disease is frequently complicated by hepatic encephalopathy (HE), hepatorenal syndrome, and spontaneous bacterial peritonitis; predictors of poor prognosis that significantly reduce survival. While orthotopic liver transplantation (OLT) remains the definitive treatment, it is often inaccessible in resource-limited settings. We present the case of a 70-year-old retired hospital attendant with hypertension who developed decompensated liver cirrhosis secondary to chronic hepatitis C virus HCV infection. She presented with portal hypertension, grade 4 HE, hepatorenal syndrome, and spontaneous bacterial peritonitis. She remained in grade 3 to 4 HE for approximately three months and in grade 2-3 HE for an additional two months. Despite profound hepatic decompensation and a high Model for End-Stage Liver Disease-Sodium (MELD-Na) score of 48 (indicating a 71% three-month mortality) and a Child-Pugh score of 15 (Class C), she responded remarkably to intensive conservative management. After six months of inpatient care, which included direct-acting antiviral therapy, anti-failure therapy, and seizure management, she recovered from hepatic coma. She received a six-month course of direct-acting antivirals (DAAs)daclatasvir and sofosbuvir and achieved sustained virologic response. Over six and a half years later, she remains in good health with preserved cognition and normal blood pressure and has been under annual surveillance for hepatocellular carcinoma. This case underscores the transformative potential of DAAs in improving survival even among severely decompensated HCV-related cirrhotic patients. It highlights the need for expanded access and subsidization of DAAs in low-resource settings, where liver transplantation is not feasible, and emphasizes the role of aggressive, supportive management in bridging the treatment gap.</p>","PeriodicalId":94346,"journal":{"name":"Nigerian medical journal : journal of the Nigeria Medical Association","volume":"66 2","pages":"791-798"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12280298/pdf/","citationCount":"0","resultStr":"{\"title\":\"An unusual survival for 6.5 years with end-stage hepatitis C related advanced liver cirrhosis following sustained virologic response with direct antiviral agents - A case report from A low-resource setting.\",\"authors\":\"Roland I Stephen, Jimmy A Reyes, Jacob A Dunga, Sati K Awang, Kefas P Zawaya\",\"doi\":\"10.71480/nmj.v66i2.661\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Advanced chronic liver disease is frequently complicated by hepatic encephalopathy (HE), hepatorenal syndrome, and spontaneous bacterial peritonitis; predictors of poor prognosis that significantly reduce survival. While orthotopic liver transplantation (OLT) remains the definitive treatment, it is often inaccessible in resource-limited settings. We present the case of a 70-year-old retired hospital attendant with hypertension who developed decompensated liver cirrhosis secondary to chronic hepatitis C virus HCV infection. She presented with portal hypertension, grade 4 HE, hepatorenal syndrome, and spontaneous bacterial peritonitis. She remained in grade 3 to 4 HE for approximately three months and in grade 2-3 HE for an additional two months. Despite profound hepatic decompensation and a high Model for End-Stage Liver Disease-Sodium (MELD-Na) score of 48 (indicating a 71% three-month mortality) and a Child-Pugh score of 15 (Class C), she responded remarkably to intensive conservative management. After six months of inpatient care, which included direct-acting antiviral therapy, anti-failure therapy, and seizure management, she recovered from hepatic coma. She received a six-month course of direct-acting antivirals (DAAs)daclatasvir and sofosbuvir and achieved sustained virologic response. Over six and a half years later, she remains in good health with preserved cognition and normal blood pressure and has been under annual surveillance for hepatocellular carcinoma. This case underscores the transformative potential of DAAs in improving survival even among severely decompensated HCV-related cirrhotic patients. It highlights the need for expanded access and subsidization of DAAs in low-resource settings, where liver transplantation is not feasible, and emphasizes the role of aggressive, supportive management in bridging the treatment gap.</p>\",\"PeriodicalId\":94346,\"journal\":{\"name\":\"Nigerian medical journal : journal of the Nigeria Medical Association\",\"volume\":\"66 2\",\"pages\":\"791-798\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12280298/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nigerian medical journal : journal of the Nigeria Medical Association\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.71480/nmj.v66i2.661\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nigerian medical journal : journal of the Nigeria Medical Association","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.71480/nmj.v66i2.661","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
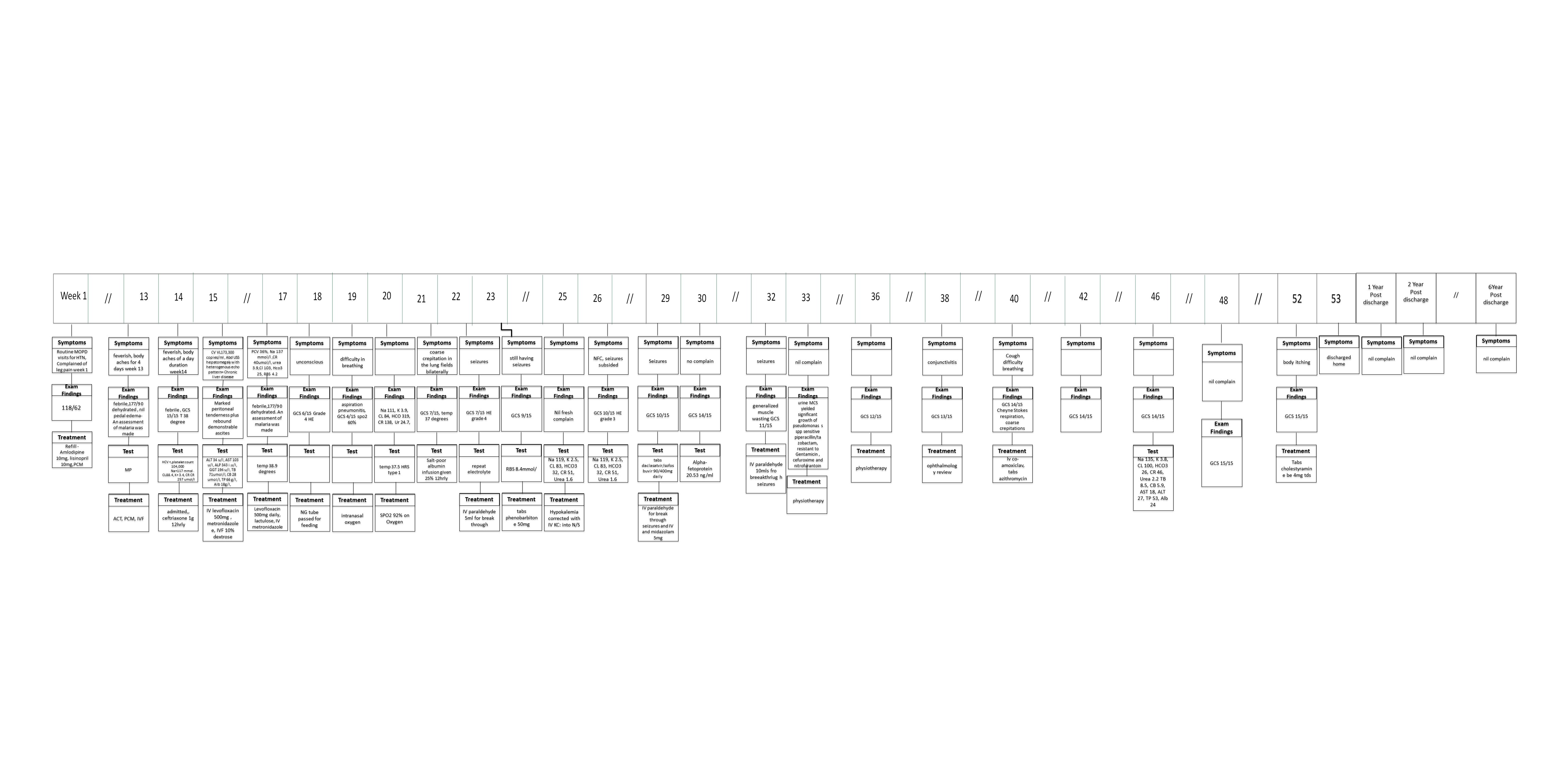
An unusual survival for 6.5 years with end-stage hepatitis C related advanced liver cirrhosis following sustained virologic response with direct antiviral agents - A case report from A low-resource setting.
Advanced chronic liver disease is frequently complicated by hepatic encephalopathy (HE), hepatorenal syndrome, and spontaneous bacterial peritonitis; predictors of poor prognosis that significantly reduce survival. While orthotopic liver transplantation (OLT) remains the definitive treatment, it is often inaccessible in resource-limited settings. We present the case of a 70-year-old retired hospital attendant with hypertension who developed decompensated liver cirrhosis secondary to chronic hepatitis C virus HCV infection. She presented with portal hypertension, grade 4 HE, hepatorenal syndrome, and spontaneous bacterial peritonitis. She remained in grade 3 to 4 HE for approximately three months and in grade 2-3 HE for an additional two months. Despite profound hepatic decompensation and a high Model for End-Stage Liver Disease-Sodium (MELD-Na) score of 48 (indicating a 71% three-month mortality) and a Child-Pugh score of 15 (Class C), she responded remarkably to intensive conservative management. After six months of inpatient care, which included direct-acting antiviral therapy, anti-failure therapy, and seizure management, she recovered from hepatic coma. She received a six-month course of direct-acting antivirals (DAAs)daclatasvir and sofosbuvir and achieved sustained virologic response. Over six and a half years later, she remains in good health with preserved cognition and normal blood pressure and has been under annual surveillance for hepatocellular carcinoma. This case underscores the transformative potential of DAAs in improving survival even among severely decompensated HCV-related cirrhotic patients. It highlights the need for expanded access and subsidization of DAAs in low-resource settings, where liver transplantation is not feasible, and emphasizes the role of aggressive, supportive management in bridging the treatment gap.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


