Mathias Klemm, Lukas von Stülpnagel, Valentin Ostermaier, Carsten Theurer, Laura E Villegas Sierra, Felix Wenner, Elodie Eiffener, Aresa Krasniqi, Konstantinos Mourouzis, Lauren E Sams, Luisa Freyer, Steffen Massberg, Axel Bauer, Konstantinos D Rizas
{"title":"心脏自主功能评分:一种基于周期性复极化动力学和心率减速能力的新型心脏重症监护病房风险分层工具(LMU-eICU研究)。","authors":"Mathias Klemm, Lukas von Stülpnagel, Valentin Ostermaier, Carsten Theurer, Laura E Villegas Sierra, Felix Wenner, Elodie Eiffener, Aresa Krasniqi, Konstantinos Mourouzis, Lauren E Sams, Luisa Freyer, Steffen Massberg, Axel Bauer, Konstantinos D Rizas","doi":"10.1093/ehjdh/ztaf038","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Treatment capacities on intensive care units (ICUs) are a limited resource reserved for high-risk patients. To facilitate risk stratification of ICU patients, several scoring systems have been developed over time. Among them, the Simplified Acute Physiology Score 3 (SAPS3) is the gold standard, but lacks specificity for cardiac ICU patients. Here, we propose a novel, fully automated, electrocardiogram-based cardiac autonomic risk stratification score (CAF<sub>ICU</sub>) that substantially adds to current risk stratification strategies.</p><p><strong>Methods and results: </strong>CAF<sub>ICU</sub> is based on periodic repolarization dynamics, a marker of sympathetic overactivity and deceleration capacity of heart rate, a parameter of vagal imbalance. We developed CAF<sub>ICU</sub> in a retrospective cohort of 355 ICU patients and subsequently validated the score in a cohort of 702 ICU patients, enrolled between February-November 2018 and December 2018-April 2020 at a large cardiac ICU in a tertiary hospital. The primary endpoint of the study was 30-day intrahospital mortality. Thirty (8.5%) and 100 (14.2%) patients reached the primary endpoint in the training and validation cohorts, respectively. CAF<sub>ICU</sub> was significantly higher in non-survivors than survivors (2.58 ± 1.34 vs. 1.76 ± 0.97 units; <i>P</i> = 0.003 in the training cohort and 2.20 ± 1.05 vs. 1.70 ± 0.83 units; <i>P</i> < 0.001 in the validation cohort) and was a strong predictor of mortality in both the training [hazard ratio (HR) 25.67; 95% confidence interval (CI) 3.50-188.40; <i>P</i> = 0.001] and validation cohorts (HR 4.70; 95% CI 2.79-7.92; <i>P</i> < 0.001). In the pooled cohort, CAF<sub>ICU</sub> significantly improved risk stratification based on SAPS3 (IDI-increase 0.033; 95% CI 0.010-0.061; <i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>ECG-based automatic autonomic risk stratification by means of PRD and DC is highly predictive of short-term mortality in the ICU and can be combined with the SAPS3-Score to identify patients with increased risk for intrahospital mortality. This method can be integrated in conventional monitors and may improve risk stratification strategies in cardiac ICUs.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 4","pages":"822-832"},"PeriodicalIF":4.4000,"publicationDate":"2025-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12282351/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cardiac autonomic function score: a novel risk stratification tool in the cardiac intensive care unit based on periodic repolarization dynamics and deceleration capacity of heart rate (LMU-eICU study).\",\"authors\":\"Mathias Klemm, Lukas von Stülpnagel, Valentin Ostermaier, Carsten Theurer, Laura E Villegas Sierra, Felix Wenner, Elodie Eiffener, Aresa Krasniqi, Konstantinos Mourouzis, Lauren E Sams, Luisa Freyer, Steffen Massberg, Axel Bauer, Konstantinos D Rizas\",\"doi\":\"10.1093/ehjdh/ztaf038\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Treatment capacities on intensive care units (ICUs) are a limited resource reserved for high-risk patients. To facilitate risk stratification of ICU patients, several scoring systems have been developed over time. Among them, the Simplified Acute Physiology Score 3 (SAPS3) is the gold standard, but lacks specificity for cardiac ICU patients. Here, we propose a novel, fully automated, electrocardiogram-based cardiac autonomic risk stratification score (CAF<sub>ICU</sub>) that substantially adds to current risk stratification strategies.</p><p><strong>Methods and results: </strong>CAF<sub>ICU</sub> is based on periodic repolarization dynamics, a marker of sympathetic overactivity and deceleration capacity of heart rate, a parameter of vagal imbalance. We developed CAF<sub>ICU</sub> in a retrospective cohort of 355 ICU patients and subsequently validated the score in a cohort of 702 ICU patients, enrolled between February-November 2018 and December 2018-April 2020 at a large cardiac ICU in a tertiary hospital. The primary endpoint of the study was 30-day intrahospital mortality. Thirty (8.5%) and 100 (14.2%) patients reached the primary endpoint in the training and validation cohorts, respectively. CAF<sub>ICU</sub> was significantly higher in non-survivors than survivors (2.58 ± 1.34 vs. 1.76 ± 0.97 units; <i>P</i> = 0.003 in the training cohort and 2.20 ± 1.05 vs. 1.70 ± 0.83 units; <i>P</i> < 0.001 in the validation cohort) and was a strong predictor of mortality in both the training [hazard ratio (HR) 25.67; 95% confidence interval (CI) 3.50-188.40; <i>P</i> = 0.001] and validation cohorts (HR 4.70; 95% CI 2.79-7.92; <i>P</i> < 0.001). In the pooled cohort, CAF<sub>ICU</sub> significantly improved risk stratification based on SAPS3 (IDI-increase 0.033; 95% CI 0.010-0.061; <i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>ECG-based automatic autonomic risk stratification by means of PRD and DC is highly predictive of short-term mortality in the ICU and can be combined with the SAPS3-Score to identify patients with increased risk for intrahospital mortality. This method can be integrated in conventional monitors and may improve risk stratification strategies in cardiac ICUs.</p>\",\"PeriodicalId\":72965,\"journal\":{\"name\":\"European heart journal. Digital health\",\"volume\":\"6 4\",\"pages\":\"822-832\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2025-04-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12282351/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal. Digital health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjdh/ztaf038\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztaf038","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
目的:重症监护病房(icu)的治疗能力是为高危患者保留的有限资源。随着时间的推移,为了促进ICU患者的风险分层,已经开发了几种评分系统。其中,简化急性生理评分3 (SAPS3)是金标准,但对心脏ICU患者缺乏特异性。在这里,我们提出了一种新颖的、全自动的、基于心电图的心脏自主风险分层评分(CAFICU),它大大增加了当前的风险分层策略。方法和结果:CAFICU基于周期性复极化动力学,是交感神经过度活跃和心率减速能力的标志,是迷走神经失衡的参数。我们在355名ICU患者的回顾性队列中开发了CAFICU,随后在702名ICU患者的队列中验证了评分,这些患者于2018年2月至11月和2018年12月至2020年4月在一家三级医院的大型心脏ICU登记。该研究的主要终点是30天院内死亡率。在训练组和验证组中,分别有30例(8.5%)和100例(14.2%)患者达到了主要终点。非幸存者的CAFICU显著高于幸存者(2.58±1.34比1.76±0.97单位;训练组P = 0.003, 2.20±1.05 vs 1.70±0.83单位;在验证队列中P < 0.001),并且在训练[危险比(HR) 25.67;95%置信区间(CI) 3.50-188.40;P = 0.001]和验证队列(HR 4.70;95% ci 2.79-7.92;P < 0.001)。在合并队列中,CAFICU显著改善了基于SAPS3的风险分层(idi增加0.033;95% ci 0.010-0.061;P < 0.001)。结论:基于心电图的PRD和DC自动自主风险分层对ICU短期死亡率具有较高的预测价值,可与SAPS3-Score联合识别院内死亡风险增高的患者。这种方法可以集成到传统的监护仪中,并可能改善心脏重症监护病房的风险分层策略。
Cardiac autonomic function score: a novel risk stratification tool in the cardiac intensive care unit based on periodic repolarization dynamics and deceleration capacity of heart rate (LMU-eICU study).
Aims: Treatment capacities on intensive care units (ICUs) are a limited resource reserved for high-risk patients. To facilitate risk stratification of ICU patients, several scoring systems have been developed over time. Among them, the Simplified Acute Physiology Score 3 (SAPS3) is the gold standard, but lacks specificity for cardiac ICU patients. Here, we propose a novel, fully automated, electrocardiogram-based cardiac autonomic risk stratification score (CAFICU) that substantially adds to current risk stratification strategies.
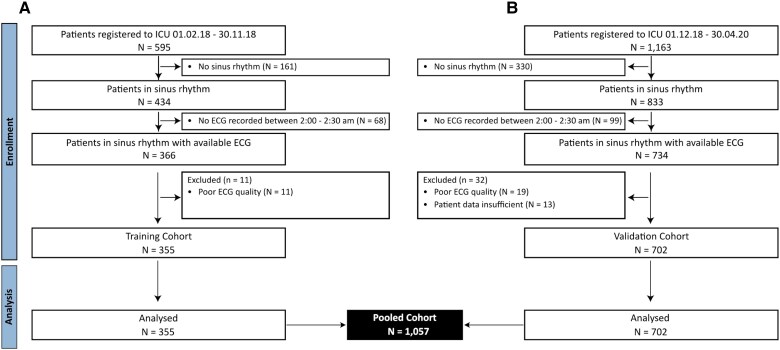
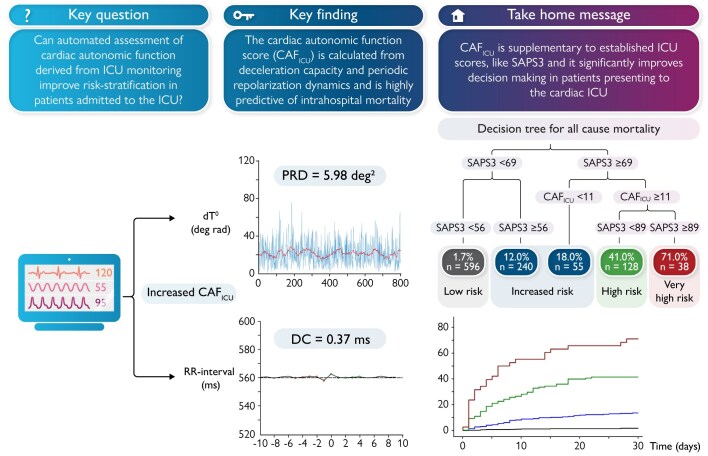
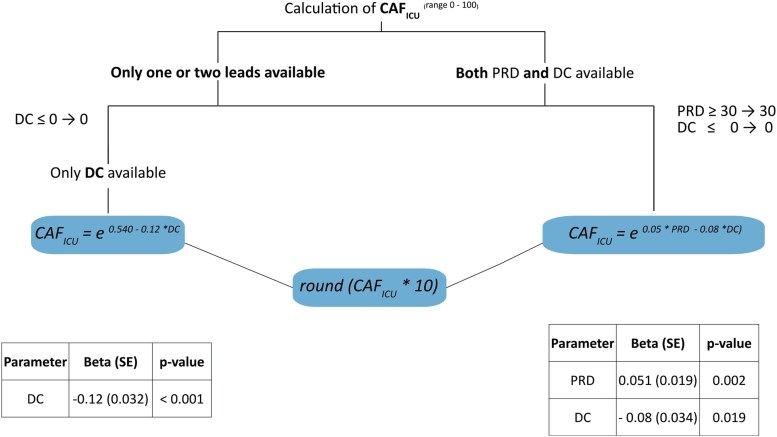
Methods and results: CAFICU is based on periodic repolarization dynamics, a marker of sympathetic overactivity and deceleration capacity of heart rate, a parameter of vagal imbalance. We developed CAFICU in a retrospective cohort of 355 ICU patients and subsequently validated the score in a cohort of 702 ICU patients, enrolled between February-November 2018 and December 2018-April 2020 at a large cardiac ICU in a tertiary hospital. The primary endpoint of the study was 30-day intrahospital mortality. Thirty (8.5%) and 100 (14.2%) patients reached the primary endpoint in the training and validation cohorts, respectively. CAFICU was significantly higher in non-survivors than survivors (2.58 ± 1.34 vs. 1.76 ± 0.97 units; P = 0.003 in the training cohort and 2.20 ± 1.05 vs. 1.70 ± 0.83 units; P < 0.001 in the validation cohort) and was a strong predictor of mortality in both the training [hazard ratio (HR) 25.67; 95% confidence interval (CI) 3.50-188.40; P = 0.001] and validation cohorts (HR 4.70; 95% CI 2.79-7.92; P < 0.001). In the pooled cohort, CAFICU significantly improved risk stratification based on SAPS3 (IDI-increase 0.033; 95% CI 0.010-0.061; P < 0.001).
Conclusion: ECG-based automatic autonomic risk stratification by means of PRD and DC is highly predictive of short-term mortality in the ICU and can be combined with the SAPS3-Score to identify patients with increased risk for intrahospital mortality. This method can be integrated in conventional monitors and may improve risk stratification strategies in cardiac ICUs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


