Justin Braver, Thomas H Marwick, Agus Salim, Dulari Hakamuwalekamlage, Catherine Keating, Stephanie R Yiallourou, Brian Oldenburg, Melinda J Carrington
{"title":"数字化心脏康复干预对危险因素、复发住院和死亡率的影响","authors":"Justin Braver, Thomas H Marwick, Agus Salim, Dulari Hakamuwalekamlage, Catherine Keating, Stephanie R Yiallourou, Brian Oldenburg, Melinda J Carrington","doi":"10.1093/ehjdh/ztaf043","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Cardiac rehabilitation (CR) programmes are effective, but they are underutilized. Digitally enabled CR programmes (DeCR) offer alternative means of healthcare delivery. We aimed to assess the effects of a DeCR programme on cardiovascular risk factors and healthcare utilization.</p><p><strong>Methods and results: </strong>In this observational cohort study that used propensity score matching, privately insured Australian patients, recruited nationally following a cardiac hospitalization, were given a digital app and received weekly telehealth consultations. Risk factors were assessed before and after the intervention. Propensity scoring methods were used to compare differences in 30-day, 90-day, and 12-month rehospitalizations, hospital-days, and mortality rates in the DeCR group with patients who undertook: (i) usual care (<i>n</i> = 266) or (ii) face-to-face CR (F2F-CR, <i>n</i> = 115). Overall, 172 intervention patients (70% men, age 68 ± 10 years, 36% living in regional/remote areas) were enrolled (59% agreed to participate and 91% completed final follow-up). The DeCR group had significant improvements in most risk factors. Rehospitalization and mortality rates were similar between the DeCR group and both comparison groups at all time points (all <i>P</i> > 0.05). Patients in the DeCR group spent significantly fewer days in hospital compared with usual care within 30-days (<i>P</i> = 0.026), 90-days (<i>P</i> = 0.003), and 12-months (<i>P</i> = 0.04) post-discharge. Cardiac-related rehospitalization bed days were reduced at 30-days (<i>P</i> = 0.005) and 90-days (<i>P</i> = 0.017) but not 12-months (<i>P</i> = 0.20). There were no group differences between DeCR and F2F-CR across any outcomes (all <i>P</i> > 0.05).</p><p><strong>Conclusion: </strong>DeCR was associated with lower healthcare utilization than usual care, yet comparable compared with F2F-CR. DeCR represents a suitable option for cardiac patients post-discharge.</p><p><strong>Lay summary: </strong>We investigated whether a digitally enabled cardiac rehabilitation (DeCR) programme, delivered to patients following a heart disease hospitalization, improved patients' cardiovascular disease risk factors and whether they had a reduction in rehospitalizations, spent fewer days in hospital and improved survival compared with matched controls who undertook either face-to-face cardiac rehabilitation (F2F-CR) or usual care.• DeCR was associated with similar healthcare utilization outcomes compared with F2F-CR. This suggests that the potential benefits of DeCR may be comparable. Additionally, DeCR programmes create an opportunity for patients to choose the style of CR to undertake and have an advantage of broader access.• The DeCR group spent significantly fewer readmission days in hospital compared with the usual care group, which may reflect differences in the nature of rehospitalizations when they occur.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 4","pages":"688-703"},"PeriodicalIF":4.4000,"publicationDate":"2025-04-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12282376/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of a digitally enabled cardiac rehabilitation intervention on risk factors, recurrent hospitalization and mortality.\",\"authors\":\"Justin Braver, Thomas H Marwick, Agus Salim, Dulari Hakamuwalekamlage, Catherine Keating, Stephanie R Yiallourou, Brian Oldenburg, Melinda J Carrington\",\"doi\":\"10.1093/ehjdh/ztaf043\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Cardiac rehabilitation (CR) programmes are effective, but they are underutilized. Digitally enabled CR programmes (DeCR) offer alternative means of healthcare delivery. We aimed to assess the effects of a DeCR programme on cardiovascular risk factors and healthcare utilization.</p><p><strong>Methods and results: </strong>In this observational cohort study that used propensity score matching, privately insured Australian patients, recruited nationally following a cardiac hospitalization, were given a digital app and received weekly telehealth consultations. Risk factors were assessed before and after the intervention. Propensity scoring methods were used to compare differences in 30-day, 90-day, and 12-month rehospitalizations, hospital-days, and mortality rates in the DeCR group with patients who undertook: (i) usual care (<i>n</i> = 266) or (ii) face-to-face CR (F2F-CR, <i>n</i> = 115). Overall, 172 intervention patients (70% men, age 68 ± 10 years, 36% living in regional/remote areas) were enrolled (59% agreed to participate and 91% completed final follow-up). The DeCR group had significant improvements in most risk factors. Rehospitalization and mortality rates were similar between the DeCR group and both comparison groups at all time points (all <i>P</i> > 0.05). Patients in the DeCR group spent significantly fewer days in hospital compared with usual care within 30-days (<i>P</i> = 0.026), 90-days (<i>P</i> = 0.003), and 12-months (<i>P</i> = 0.04) post-discharge. Cardiac-related rehospitalization bed days were reduced at 30-days (<i>P</i> = 0.005) and 90-days (<i>P</i> = 0.017) but not 12-months (<i>P</i> = 0.20). There were no group differences between DeCR and F2F-CR across any outcomes (all <i>P</i> > 0.05).</p><p><strong>Conclusion: </strong>DeCR was associated with lower healthcare utilization than usual care, yet comparable compared with F2F-CR. DeCR represents a suitable option for cardiac patients post-discharge.</p><p><strong>Lay summary: </strong>We investigated whether a digitally enabled cardiac rehabilitation (DeCR) programme, delivered to patients following a heart disease hospitalization, improved patients' cardiovascular disease risk factors and whether they had a reduction in rehospitalizations, spent fewer days in hospital and improved survival compared with matched controls who undertook either face-to-face cardiac rehabilitation (F2F-CR) or usual care.• DeCR was associated with similar healthcare utilization outcomes compared with F2F-CR. This suggests that the potential benefits of DeCR may be comparable. Additionally, DeCR programmes create an opportunity for patients to choose the style of CR to undertake and have an advantage of broader access.• The DeCR group spent significantly fewer readmission days in hospital compared with the usual care group, which may reflect differences in the nature of rehospitalizations when they occur.</p>\",\"PeriodicalId\":72965,\"journal\":{\"name\":\"European heart journal. Digital health\",\"volume\":\"6 4\",\"pages\":\"688-703\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2025-04-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12282376/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal. Digital health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjdh/ztaf043\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztaf043","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Effects of a digitally enabled cardiac rehabilitation intervention on risk factors, recurrent hospitalization and mortality.
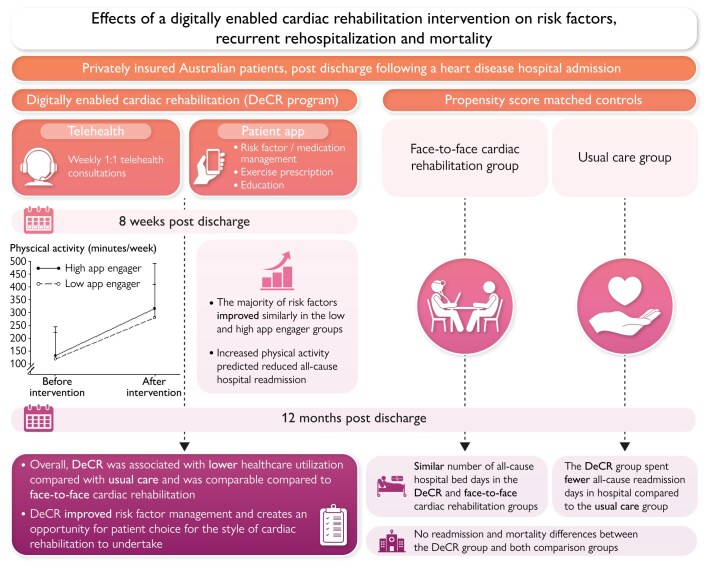
Aims: Cardiac rehabilitation (CR) programmes are effective, but they are underutilized. Digitally enabled CR programmes (DeCR) offer alternative means of healthcare delivery. We aimed to assess the effects of a DeCR programme on cardiovascular risk factors and healthcare utilization.
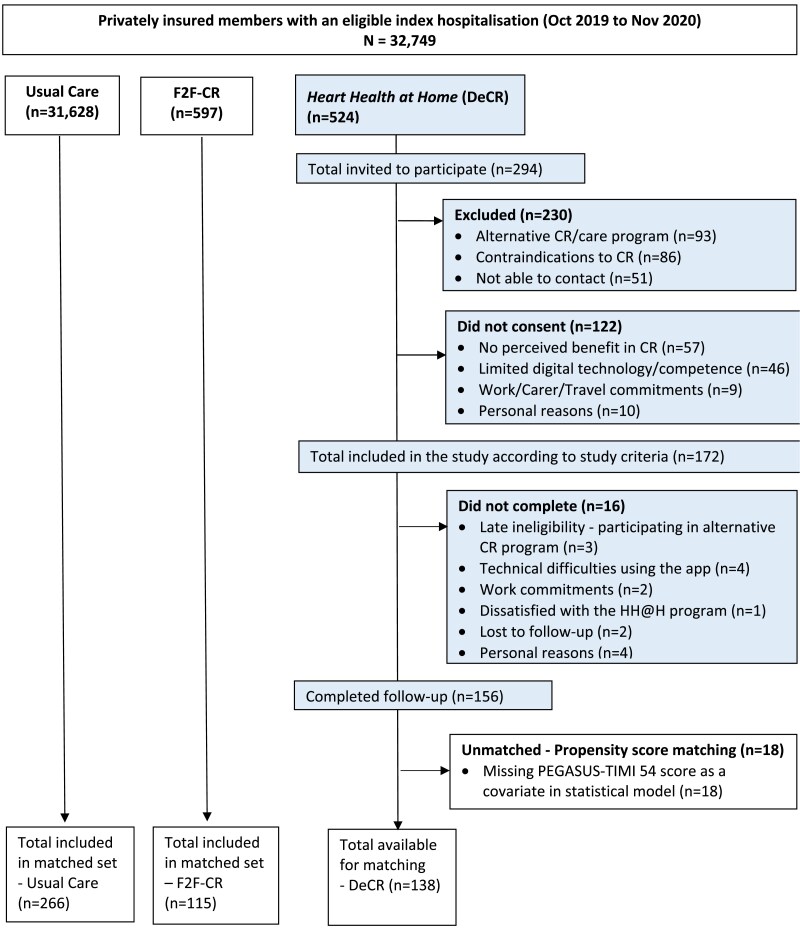
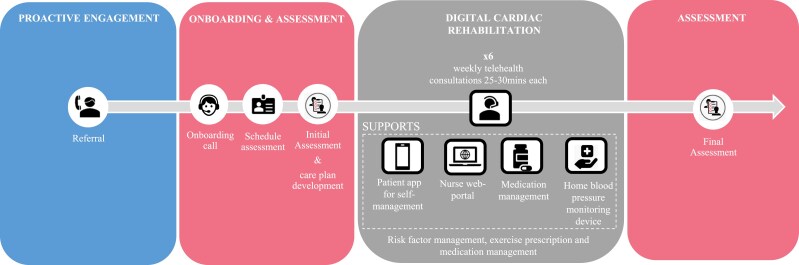
Methods and results: In this observational cohort study that used propensity score matching, privately insured Australian patients, recruited nationally following a cardiac hospitalization, were given a digital app and received weekly telehealth consultations. Risk factors were assessed before and after the intervention. Propensity scoring methods were used to compare differences in 30-day, 90-day, and 12-month rehospitalizations, hospital-days, and mortality rates in the DeCR group with patients who undertook: (i) usual care (n = 266) or (ii) face-to-face CR (F2F-CR, n = 115). Overall, 172 intervention patients (70% men, age 68 ± 10 years, 36% living in regional/remote areas) were enrolled (59% agreed to participate and 91% completed final follow-up). The DeCR group had significant improvements in most risk factors. Rehospitalization and mortality rates were similar between the DeCR group and both comparison groups at all time points (all P > 0.05). Patients in the DeCR group spent significantly fewer days in hospital compared with usual care within 30-days (P = 0.026), 90-days (P = 0.003), and 12-months (P = 0.04) post-discharge. Cardiac-related rehospitalization bed days were reduced at 30-days (P = 0.005) and 90-days (P = 0.017) but not 12-months (P = 0.20). There were no group differences between DeCR and F2F-CR across any outcomes (all P > 0.05).
Conclusion: DeCR was associated with lower healthcare utilization than usual care, yet comparable compared with F2F-CR. DeCR represents a suitable option for cardiac patients post-discharge.
Lay summary: We investigated whether a digitally enabled cardiac rehabilitation (DeCR) programme, delivered to patients following a heart disease hospitalization, improved patients' cardiovascular disease risk factors and whether they had a reduction in rehospitalizations, spent fewer days in hospital and improved survival compared with matched controls who undertook either face-to-face cardiac rehabilitation (F2F-CR) or usual care.• DeCR was associated with similar healthcare utilization outcomes compared with F2F-CR. This suggests that the potential benefits of DeCR may be comparable. Additionally, DeCR programmes create an opportunity for patients to choose the style of CR to undertake and have an advantage of broader access.• The DeCR group spent significantly fewer readmission days in hospital compared with the usual care group, which may reflect differences in the nature of rehospitalizations when they occur.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


