Fahim Kanani, Ester Ovdat, Mohammed Younis, Guy Meyerovich, Nir Messer, Alexander Barenboim, Yaacov Goykhman, Nir Lubezky
{"title":"新辅助FOLFIRINOX后胰腺切除术合并动脉切除术:单一机构的经验。","authors":"Fahim Kanani, Ester Ovdat, Mohammed Younis, Guy Meyerovich, Nir Messer, Alexander Barenboim, Yaacov Goykhman, Nir Lubezky","doi":"10.14701/ahbps.25-108","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>Arterial resection in pancreatic cancer remains controversial. This study evaluates outcomes of pancreatic resection with arterial involvement following neoadjuvant chemotherapy.</p><p><strong>Methods: </strong>Retrospective analysis of 100 pancreatic adenocarcinoma patients undergoing resection after neoadjuvant FOLFIRINOX (2010-2024): 26 with arterial resection (ArP), 39 with portal-venous resection (PoP), and 35 without vascular involvement (NoP). Primary outcomes included perioperative morbidity, mortality, and survival.</p><p><strong>Results: </strong>ArP patients had significantly more stage III disease (73.1% vs 58.9% vs 28.6%, <i>p</i> < 0.001) but achieved acceptable R0 resection rates (76.9% vs 84.6% vs 91.4%, <i>p</i> = 0.04). ArP procedures required longer operative time (386 ± 71 minutes), greater blood loss (1,100 ± 560 mL), and more transfusions (57.7%; all <i>p</i> < 0.001). Major complications (Clavien-Dindo ≥ III) were higher in ArP (26.9% vs 21.6% vs 8.6%, <i>p</i> = 0.03), with extended ICU stays (3.5 ± 1.5 vs 2.0 ± 1.0 vs 1.0 ± 0.5 days). Ninety-day mortality was 0% (ArP), 2.5% (PoP), and 5.7% (NoP) (<i>p</i> = 0.78). Despite shorter disease-free survival in ArP (7.4 vs 9.7 vs 13.2 months, <i>p</i> = 0.01), median overall survival was comparable (ArP: 19.1, PoP: 18.3, NoP: 22.7 months; <i>p</i> = 0.0652).</p><p><strong>Conclusions: </strong>Arterial resection following neoadjuvant therapy in selected pancreatic cancer patients demonstrates acceptable perioperative risk and achieves survival outcomes comparable to less advanced cases. This approach is justified in experienced high-volume centers for appropriately selected patients with favorable response to neoadjuvant therapy, offering potential cure in rare circumstances.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"323-333"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377994/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pancreatectomy with arterial resection following neoadjuvant FOLFIRINOX: A single-institution experience.\",\"authors\":\"Fahim Kanani, Ester Ovdat, Mohammed Younis, Guy Meyerovich, Nir Messer, Alexander Barenboim, Yaacov Goykhman, Nir Lubezky\",\"doi\":\"10.14701/ahbps.25-108\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Backgrounds/aims: </strong>Arterial resection in pancreatic cancer remains controversial. This study evaluates outcomes of pancreatic resection with arterial involvement following neoadjuvant chemotherapy.</p><p><strong>Methods: </strong>Retrospective analysis of 100 pancreatic adenocarcinoma patients undergoing resection after neoadjuvant FOLFIRINOX (2010-2024): 26 with arterial resection (ArP), 39 with portal-venous resection (PoP), and 35 without vascular involvement (NoP). Primary outcomes included perioperative morbidity, mortality, and survival.</p><p><strong>Results: </strong>ArP patients had significantly more stage III disease (73.1% vs 58.9% vs 28.6%, <i>p</i> < 0.001) but achieved acceptable R0 resection rates (76.9% vs 84.6% vs 91.4%, <i>p</i> = 0.04). ArP procedures required longer operative time (386 ± 71 minutes), greater blood loss (1,100 ± 560 mL), and more transfusions (57.7%; all <i>p</i> < 0.001). Major complications (Clavien-Dindo ≥ III) were higher in ArP (26.9% vs 21.6% vs 8.6%, <i>p</i> = 0.03), with extended ICU stays (3.5 ± 1.5 vs 2.0 ± 1.0 vs 1.0 ± 0.5 days). Ninety-day mortality was 0% (ArP), 2.5% (PoP), and 5.7% (NoP) (<i>p</i> = 0.78). Despite shorter disease-free survival in ArP (7.4 vs 9.7 vs 13.2 months, <i>p</i> = 0.01), median overall survival was comparable (ArP: 19.1, PoP: 18.3, NoP: 22.7 months; <i>p</i> = 0.0652).</p><p><strong>Conclusions: </strong>Arterial resection following neoadjuvant therapy in selected pancreatic cancer patients demonstrates acceptable perioperative risk and achieves survival outcomes comparable to less advanced cases. This approach is justified in experienced high-volume centers for appropriately selected patients with favorable response to neoadjuvant therapy, offering potential cure in rare circumstances.</p>\",\"PeriodicalId\":72220,\"journal\":{\"name\":\"Annals of hepato-biliary-pancreatic surgery\",\"volume\":\" \",\"pages\":\"323-333\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-08-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377994/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of hepato-biliary-pancreatic surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14701/ahbps.25-108\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.25-108","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/24 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景/目的:胰腺癌的动脉切除术仍然存在争议。本研究评估新辅助化疗后动脉受累胰腺切除术的预后。方法:回顾性分析2010-2024年接受新辅助FOLFIRINOX手术的100例胰腺癌患者,其中动脉切除术(ArP) 26例,门静脉切除术(PoP) 39例,不累及血管(NoP) 35例。主要结局包括围手术期发病率、死亡率和生存率。结果:ArP患者有更多的III期疾病(73.1% vs 58.9% vs 28.6%, p < 0.001),但获得了可接受的R0切除率(76.9% vs 84.6% vs 91.4%, p = 0.04)。ArP手术需要更长的手术时间(386±71分钟),更大的失血量(1100±560毫升),更多的输血(57.7%;均p < 0.001)。ArP组的主要并发症(Clavien-Dindo≥III)较高(26.9% vs 21.6% vs 8.6%, p = 0.03), ICU住院时间延长(3.5±1.5 vs 2.0±1.0 vs 1.0±0.5 d)。90天死亡率分别为0% (ArP)、2.5% (PoP)和5.7% (NoP) (p = 0.78)。尽管ArP组无病生存期较短(7.4个月vs 9.7个月vs 13.2个月,p = 0.01),但中位总生存期相当(ArP: 19.1个月,PoP: 18.3个月,NoP: 22.7个月;P = 0.0652)。结论:选定的胰腺癌患者在新辅助治疗后进行动脉切除,围手术期风险可接受,生存结果与较不晚期的病例相当。这种方法在经验丰富的大容量中心被证明是合理的,用于适当选择对新辅助治疗有良好反应的患者,在罕见的情况下提供潜在的治愈。
Pancreatectomy with arterial resection following neoadjuvant FOLFIRINOX: A single-institution experience.
Backgrounds/aims: Arterial resection in pancreatic cancer remains controversial. This study evaluates outcomes of pancreatic resection with arterial involvement following neoadjuvant chemotherapy.
Methods: Retrospective analysis of 100 pancreatic adenocarcinoma patients undergoing resection after neoadjuvant FOLFIRINOX (2010-2024): 26 with arterial resection (ArP), 39 with portal-venous resection (PoP), and 35 without vascular involvement (NoP). Primary outcomes included perioperative morbidity, mortality, and survival.
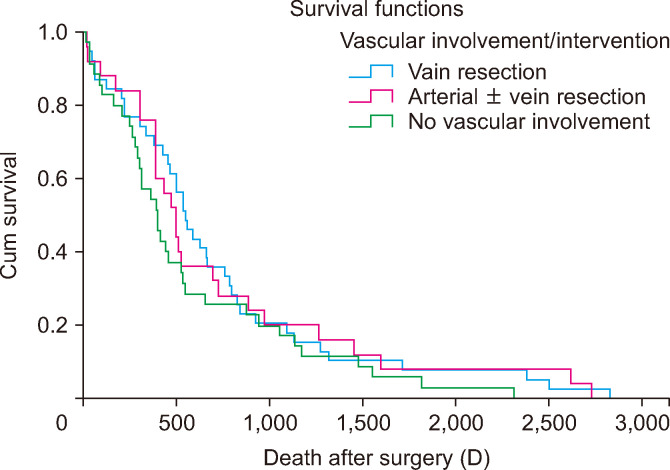
Results: ArP patients had significantly more stage III disease (73.1% vs 58.9% vs 28.6%, p < 0.001) but achieved acceptable R0 resection rates (76.9% vs 84.6% vs 91.4%, p = 0.04). ArP procedures required longer operative time (386 ± 71 minutes), greater blood loss (1,100 ± 560 mL), and more transfusions (57.7%; all p < 0.001). Major complications (Clavien-Dindo ≥ III) were higher in ArP (26.9% vs 21.6% vs 8.6%, p = 0.03), with extended ICU stays (3.5 ± 1.5 vs 2.0 ± 1.0 vs 1.0 ± 0.5 days). Ninety-day mortality was 0% (ArP), 2.5% (PoP), and 5.7% (NoP) (p = 0.78). Despite shorter disease-free survival in ArP (7.4 vs 9.7 vs 13.2 months, p = 0.01), median overall survival was comparable (ArP: 19.1, PoP: 18.3, NoP: 22.7 months; p = 0.0652).
Conclusions: Arterial resection following neoadjuvant therapy in selected pancreatic cancer patients demonstrates acceptable perioperative risk and achieves survival outcomes comparable to less advanced cases. This approach is justified in experienced high-volume centers for appropriately selected patients with favorable response to neoadjuvant therapy, offering potential cure in rare circumstances.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


