{"title":"美国老年人适应负荷与多发病的纵向关系。","authors":"Rolla Mira, Jonathon Timothy Newton, Wael Sabbah","doi":"10.3390/geriatrics10040084","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> To examine the association between allostatic load and the progression of multimorbidity and the role of socioeconomic factors among older Americans. <b>Methods:</b> Data from the Health and Retirement Study (HRS), a longitudinal study of older American adults, were used. Data were included from waves 8 (2006), 10 (2010), 11 (2012), and 13 (2016). Self-reported diagnoses of five chronic conditions (diabetes, heart disease, lung diseases, cancer, and stroke) indicated multimorbidity and were dichotomised to reflect having two or more conditions versus one or fewer. Multimorbidity in 2006 was subtracted from that in 2016 to calculate ten-year change in multimorbidity. Sociodemographic data (age, gender, education, and wealth) were from wave 8 (2006). Behaviours (physical activity and smoking) were from wave 10 (2010). Allostatic load, indicated by five biomarkers (waist circumference, high blood pressure, glycosylated haemoglobin, high-density lipoprotein, and c-reactive protein), was from wave 11 (2012). Structural Equation Modelling (SEM) was used to assess the longitudinal association between the aforementioned factors and the incidence of multimorbidity in 2016. Results: Given that allostatic load was assessed in a subsample of HRS, 8222 were excluded for lack of relevant data. A total of 3336 participants were included in the final analysis. The incidence of multimorbidity in 2016 was 19%. Allostatic load in 2012 was significantly associated with the incidence of multimorbidity in 2016 (estimate 0.10, 95% Confidence Interval (CI) 0.07, 0.14); in other words, for an additional marker of allostatic load, there was an average 0.1 change in the incidence of multimorbidity. Wealth and education (2006) were indirectly associated with multimorbidity through allostatic load and behaviours. Smoking (2010) was positively associated with multimorbidity in 2016, while physical activity showed a negative association. <b>Conclusions:</b> Biological markers of stress indicated by allostatic load were associated with multimorbidity. Adverse socioeconomic conditions appear to induce allostatic load and risk behaviours, which impact the progression of multimorbidity.</p>","PeriodicalId":12653,"journal":{"name":"Geriatrics","volume":"10 4","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2025-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12286139/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Longitudinal Relationship Between Allostatic Load and Multimorbidity Among Older Americans.\",\"authors\":\"Rolla Mira, Jonathon Timothy Newton, Wael Sabbah\",\"doi\":\"10.3390/geriatrics10040084\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> To examine the association between allostatic load and the progression of multimorbidity and the role of socioeconomic factors among older Americans. <b>Methods:</b> Data from the Health and Retirement Study (HRS), a longitudinal study of older American adults, were used. Data were included from waves 8 (2006), 10 (2010), 11 (2012), and 13 (2016). Self-reported diagnoses of five chronic conditions (diabetes, heart disease, lung diseases, cancer, and stroke) indicated multimorbidity and were dichotomised to reflect having two or more conditions versus one or fewer. Multimorbidity in 2006 was subtracted from that in 2016 to calculate ten-year change in multimorbidity. Sociodemographic data (age, gender, education, and wealth) were from wave 8 (2006). Behaviours (physical activity and smoking) were from wave 10 (2010). Allostatic load, indicated by five biomarkers (waist circumference, high blood pressure, glycosylated haemoglobin, high-density lipoprotein, and c-reactive protein), was from wave 11 (2012). Structural Equation Modelling (SEM) was used to assess the longitudinal association between the aforementioned factors and the incidence of multimorbidity in 2016. Results: Given that allostatic load was assessed in a subsample of HRS, 8222 were excluded for lack of relevant data. A total of 3336 participants were included in the final analysis. The incidence of multimorbidity in 2016 was 19%. Allostatic load in 2012 was significantly associated with the incidence of multimorbidity in 2016 (estimate 0.10, 95% Confidence Interval (CI) 0.07, 0.14); in other words, for an additional marker of allostatic load, there was an average 0.1 change in the incidence of multimorbidity. Wealth and education (2006) were indirectly associated with multimorbidity through allostatic load and behaviours. Smoking (2010) was positively associated with multimorbidity in 2016, while physical activity showed a negative association. <b>Conclusions:</b> Biological markers of stress indicated by allostatic load were associated with multimorbidity. Adverse socioeconomic conditions appear to induce allostatic load and risk behaviours, which impact the progression of multimorbidity.</p>\",\"PeriodicalId\":12653,\"journal\":{\"name\":\"Geriatrics\",\"volume\":\"10 4\",\"pages\":\"\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-06-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12286139/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Geriatrics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/geriatrics10040084\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Geriatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/geriatrics10040084","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
The Longitudinal Relationship Between Allostatic Load and Multimorbidity Among Older Americans.
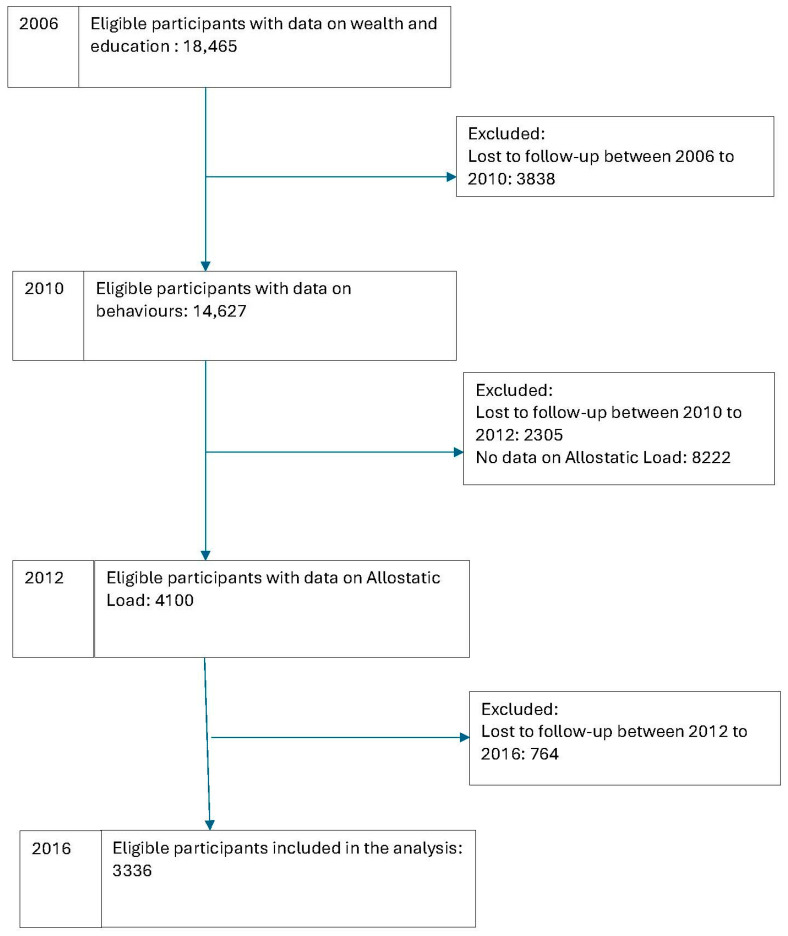
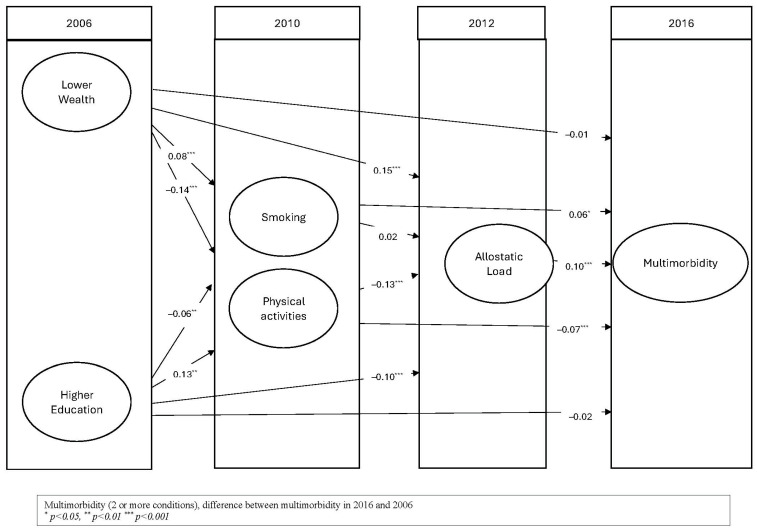
Background: To examine the association between allostatic load and the progression of multimorbidity and the role of socioeconomic factors among older Americans. Methods: Data from the Health and Retirement Study (HRS), a longitudinal study of older American adults, were used. Data were included from waves 8 (2006), 10 (2010), 11 (2012), and 13 (2016). Self-reported diagnoses of five chronic conditions (diabetes, heart disease, lung diseases, cancer, and stroke) indicated multimorbidity and were dichotomised to reflect having two or more conditions versus one or fewer. Multimorbidity in 2006 was subtracted from that in 2016 to calculate ten-year change in multimorbidity. Sociodemographic data (age, gender, education, and wealth) were from wave 8 (2006). Behaviours (physical activity and smoking) were from wave 10 (2010). Allostatic load, indicated by five biomarkers (waist circumference, high blood pressure, glycosylated haemoglobin, high-density lipoprotein, and c-reactive protein), was from wave 11 (2012). Structural Equation Modelling (SEM) was used to assess the longitudinal association between the aforementioned factors and the incidence of multimorbidity in 2016. Results: Given that allostatic load was assessed in a subsample of HRS, 8222 were excluded for lack of relevant data. A total of 3336 participants were included in the final analysis. The incidence of multimorbidity in 2016 was 19%. Allostatic load in 2012 was significantly associated with the incidence of multimorbidity in 2016 (estimate 0.10, 95% Confidence Interval (CI) 0.07, 0.14); in other words, for an additional marker of allostatic load, there was an average 0.1 change in the incidence of multimorbidity. Wealth and education (2006) were indirectly associated with multimorbidity through allostatic load and behaviours. Smoking (2010) was positively associated with multimorbidity in 2016, while physical activity showed a negative association. Conclusions: Biological markers of stress indicated by allostatic load were associated with multimorbidity. Adverse socioeconomic conditions appear to induce allostatic load and risk behaviours, which impact the progression of multimorbidity.
期刊介绍:
• Geriatric biology
• Geriatric health services research
• Geriatric medicine research
• Geriatric neurology, stroke, cognition and oncology
• Geriatric surgery
• Geriatric physical functioning, physical health and activity
• Geriatric psychiatry and psychology
• Geriatric nutrition
• Geriatric epidemiology
• Geriatric rehabilitation

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


