Aziz Zaanan, Audrey Didelot, Chloé Broudin, George Laliotis, Erik Spickard, Punashi Dutta, Aurélien Saltel-Fulero, Francesco Giulio Sullo, Margot Pizzamiglio, Antoine Mariani, Widad Lahlou, Meenakshi Malhotra, Shruti Sharma, Himanshu Sethi, Adham Jurdi, Minetta C. Liu, Pierre Laurent-Puig
{"title":"局部晚期可切除胃或胃食管交界处腺癌治疗期间的纵向循环肿瘤DNA分析:PLAGAST前瞻性生物标志物研究","authors":"Aziz Zaanan, Audrey Didelot, Chloé Broudin, George Laliotis, Erik Spickard, Punashi Dutta, Aurélien Saltel-Fulero, Francesco Giulio Sullo, Margot Pizzamiglio, Antoine Mariani, Widad Lahlou, Meenakshi Malhotra, Shruti Sharma, Himanshu Sethi, Adham Jurdi, Minetta C. Liu, Pierre Laurent-Puig","doi":"10.1038/s41467-025-62056-7","DOIUrl":null,"url":null,"abstract":"<p>Patients with locally advanced resectable (LAR) gastric/gastroesophageal junction (G/GEJ) adenocarcinomas have a high recurrence risk despite pre- and post-operative treatment. In the PLAGAST prospective study (NCT02674373), we investigated the ability of circulating tumor DNA (ctDNA) to predict treatment response and improve risk stratification. Plasma samples were prospectively collected before neoadjuvant therapy (NAT), during-NAT, post-NAT, and post-surgery. The primary endpoint was recurrence-free survival (RFS), and the secondary endpoints were overall survival (OS), tumor regression grade (TRG), and pathological tumor stage. ctDNA positivity decreased over these four therapeutic timelines (69.6%, 51.2%, 26.8%, and 20%, respectively). ctDNA-positivity was associated with significantly worse outcomes during-NAT (RFS: HR = 6.17, <i>P</i> = 0.002; OS: HR = 4.71, <i>P</i> = 0.022), post-NAT (RFS: HR = 5.26, <i>P</i> = 0.001; OS: HR = 7.35, <i>P</i> = 0.001) and after surgery (RFS: HR = 12.94, <i>P</i> < 0.0001; OS: HR = 14.54, <i>P</i> < 0.0001). Patients with early ctDNA clearance during NAT had better outcomes compared to those who cleared ctDNA post-NAT, while patients who remained ctDNA-positive pre-, during-, and post-NAT had worse outcomes (RFS: HR = 18.57, <i>P</i> = 0.01; OS: HR = 16.06, <i>P</i> = 0.007). Our data suggests that longitudinal ctDNA monitoring is prognostic of patient outcomes and may guide therapeutic decision-making in patients with LAR G/GEJ adenocarcinoma.</p>","PeriodicalId":19066,"journal":{"name":"Nature Communications","volume":"143 1","pages":""},"PeriodicalIF":15.7000,"publicationDate":"2025-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Longitudinal circulating tumor DNA analysis during treatment of locally advanced resectable gastric or gastroesophageal junction adenocarcinoma: the PLAGAST prospective biomarker study\",\"authors\":\"Aziz Zaanan, Audrey Didelot, Chloé Broudin, George Laliotis, Erik Spickard, Punashi Dutta, Aurélien Saltel-Fulero, Francesco Giulio Sullo, Margot Pizzamiglio, Antoine Mariani, Widad Lahlou, Meenakshi Malhotra, Shruti Sharma, Himanshu Sethi, Adham Jurdi, Minetta C. Liu, Pierre Laurent-Puig\",\"doi\":\"10.1038/s41467-025-62056-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Patients with locally advanced resectable (LAR) gastric/gastroesophageal junction (G/GEJ) adenocarcinomas have a high recurrence risk despite pre- and post-operative treatment. In the PLAGAST prospective study (NCT02674373), we investigated the ability of circulating tumor DNA (ctDNA) to predict treatment response and improve risk stratification. Plasma samples were prospectively collected before neoadjuvant therapy (NAT), during-NAT, post-NAT, and post-surgery. The primary endpoint was recurrence-free survival (RFS), and the secondary endpoints were overall survival (OS), tumor regression grade (TRG), and pathological tumor stage. ctDNA positivity decreased over these four therapeutic timelines (69.6%, 51.2%, 26.8%, and 20%, respectively). ctDNA-positivity was associated with significantly worse outcomes during-NAT (RFS: HR = 6.17, <i>P</i> = 0.002; OS: HR = 4.71, <i>P</i> = 0.022), post-NAT (RFS: HR = 5.26, <i>P</i> = 0.001; OS: HR = 7.35, <i>P</i> = 0.001) and after surgery (RFS: HR = 12.94, <i>P</i> < 0.0001; OS: HR = 14.54, <i>P</i> < 0.0001). Patients with early ctDNA clearance during NAT had better outcomes compared to those who cleared ctDNA post-NAT, while patients who remained ctDNA-positive pre-, during-, and post-NAT had worse outcomes (RFS: HR = 18.57, <i>P</i> = 0.01; OS: HR = 16.06, <i>P</i> = 0.007). Our data suggests that longitudinal ctDNA monitoring is prognostic of patient outcomes and may guide therapeutic decision-making in patients with LAR G/GEJ adenocarcinoma.</p>\",\"PeriodicalId\":19066,\"journal\":{\"name\":\"Nature Communications\",\"volume\":\"143 1\",\"pages\":\"\"},\"PeriodicalIF\":15.7000,\"publicationDate\":\"2025-07-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nature Communications\",\"FirstCategoryId\":\"103\",\"ListUrlMain\":\"https://doi.org/10.1038/s41467-025-62056-7\",\"RegionNum\":1,\"RegionCategory\":\"综合性期刊\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature Communications","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1038/s41467-025-62056-7","RegionNum":1,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
摘要
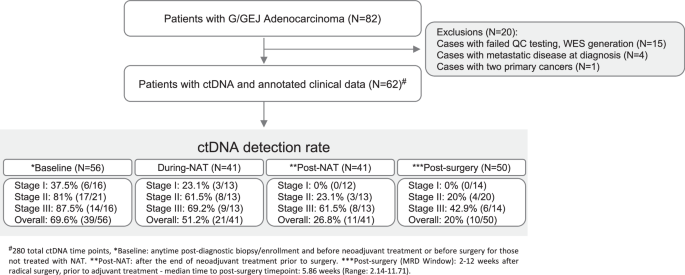
局部晚期可切除(LAR)胃/胃食管交界处(G/GEJ)腺癌患者尽管进行了术前和术后治疗,但仍有很高的复发风险。在PLAGAST前瞻性研究(NCT02674373)中,我们研究了循环肿瘤DNA (ctDNA)预测治疗反应和改善风险分层的能力。在新辅助治疗(NAT)前、NAT中、NAT后和手术后前瞻性采集血浆样本。主要终点为无复发生存期(RFS),次要终点为总生存期(OS)、肿瘤消退等级(TRG)和肿瘤病理分期。ctDNA阳性在这四个治疗时间内分别下降了69.6%、51.2%、26.8%和20%。ctdna阳性与nat期间预后显著差相关(RFS: HR = 6.17, P = 0.002;操作系统:HR = 4.71, P = 0.022), post-NAT (RFS: HR = 5.26, P = 0.001;操作系统:HR = 7.35, P = 0.001)和手术后(RFS: HR = 12.94, P & lt; 0.0001;OS: HR = 14.54, P < 0.0001)。与NAT后清除ctDNA的患者相比,NAT期间早期ctDNA清除的患者预后较好,而NAT前、NAT中和NAT后ctDNA阳性的患者预后较差(RFS: HR = 18.57, P = 0.01;Os: hr = 16.06, p = 0.007)。我们的数据表明,纵向ctDNA监测可预测患者预后,并可指导LAR G/GEJ腺癌患者的治疗决策。
Longitudinal circulating tumor DNA analysis during treatment of locally advanced resectable gastric or gastroesophageal junction adenocarcinoma: the PLAGAST prospective biomarker study
Patients with locally advanced resectable (LAR) gastric/gastroesophageal junction (G/GEJ) adenocarcinomas have a high recurrence risk despite pre- and post-operative treatment. In the PLAGAST prospective study (NCT02674373), we investigated the ability of circulating tumor DNA (ctDNA) to predict treatment response and improve risk stratification. Plasma samples were prospectively collected before neoadjuvant therapy (NAT), during-NAT, post-NAT, and post-surgery. The primary endpoint was recurrence-free survival (RFS), and the secondary endpoints were overall survival (OS), tumor regression grade (TRG), and pathological tumor stage. ctDNA positivity decreased over these four therapeutic timelines (69.6%, 51.2%, 26.8%, and 20%, respectively). ctDNA-positivity was associated with significantly worse outcomes during-NAT (RFS: HR = 6.17, P = 0.002; OS: HR = 4.71, P = 0.022), post-NAT (RFS: HR = 5.26, P = 0.001; OS: HR = 7.35, P = 0.001) and after surgery (RFS: HR = 12.94, P < 0.0001; OS: HR = 14.54, P < 0.0001). Patients with early ctDNA clearance during NAT had better outcomes compared to those who cleared ctDNA post-NAT, while patients who remained ctDNA-positive pre-, during-, and post-NAT had worse outcomes (RFS: HR = 18.57, P = 0.01; OS: HR = 16.06, P = 0.007). Our data suggests that longitudinal ctDNA monitoring is prognostic of patient outcomes and may guide therapeutic decision-making in patients with LAR G/GEJ adenocarcinoma.
期刊介绍:
Nature Communications, an open-access journal, publishes high-quality research spanning all areas of the natural sciences. Papers featured in the journal showcase significant advances relevant to specialists in each respective field. With a 2-year impact factor of 16.6 (2022) and a median time of 8 days from submission to the first editorial decision, Nature Communications is committed to rapid dissemination of research findings. As a multidisciplinary journal, it welcomes contributions from biological, health, physical, chemical, Earth, social, mathematical, applied, and engineering sciences, aiming to highlight important breakthroughs within each domain.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


