{"title":"圆锥角膜的标准交联和加速交联:一年内的差异和进化。","authors":"Maria-Silvia Dina, Mihaela-Monica Constantin, Maria-Cristina Marinescu, Cătălina-Gabriela Corbu, Cătălina-Ioana Tătaru, Călin-Petru Tătaru","doi":"10.22336/rjo.2025.29","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Keratoconus (KC) is a bilateral, progressive corneal ectasia that involves corneal thinning and a decrease in visual acuity. Stopping the progression of keratoconus can be achieved through various photooxidative crosslinking (CXL) methods. The objective of this study was to compare two protocols of epi-off corneal crosslinking-the standard and the accelerated protocol-in terms of efficacy after a one-year follow-up.</p><p><strong>Methods: </strong>41 eyes with progressive keratoconus were treated with corneal crosslinking, either using the accelerated (Acc-CXL) or standard protocol (Std-CXL). The following parameters were monitored: refraction, corneal diopter power on topographic maps (Kmax and Kmin), corneal thickness (CCT), resistance factor (CRF), hysteresis, and the depth of the demarcation line. All measurements were repeated 12 months after the intervention.</p><p><strong>Results: </strong>The progression of keratoconus was halted in 20 eyes using the accelerated method and in 21 eyes using the standard procedure. Both methods resulted in a statistically significant regression of the spherical equivalent, Kmax, and an increase in CCT and CRF, without substantial differences in efficacy. The demarcation line was highlighted on average at a depth of 278.9 ± 31.71 micrometres for the Acc-CXL group and 280.42 ± 47.85 micrometres for the Std-CXL group. It was correlated with the initial topographical values.</p><p><strong>Discussion: </strong>The evaluation of patients revealed no progression of keratoconus following the procedure. Approximately 40% of the cases in the accelerated protocol group and 38.09% of the cases in the standard protocol group have maintained the parameters at a constant level. In comparison, approximately 60% of the cases have shown improvements. An Australian registry revealed that both CXL protocols are safe and effective; however, the standard procedure leads to improved visual acuity, a more significant flattening of the steepest meridian, and a higher chance of an effect greater than one diopter power.</p><p><strong>Conclusions: </strong>Corneal crosslinking (CXL) was effective in halting the progression of keratoconus using both methods. Accelerated CXL is faster and more comfortable for patients, with similar efficiency to standard CXL.</p>","PeriodicalId":94355,"journal":{"name":"Romanian journal of ophthalmology","volume":"69 2","pages":"175-183"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12277981/pdf/","citationCount":"0","resultStr":"{\"title\":\"Standard and accelerated crosslinking protocols in keratoconus - differences and evolution at one year.\",\"authors\":\"Maria-Silvia Dina, Mihaela-Monica Constantin, Maria-Cristina Marinescu, Cătălina-Gabriela Corbu, Cătălina-Ioana Tătaru, Călin-Petru Tătaru\",\"doi\":\"10.22336/rjo.2025.29\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Keratoconus (KC) is a bilateral, progressive corneal ectasia that involves corneal thinning and a decrease in visual acuity. Stopping the progression of keratoconus can be achieved through various photooxidative crosslinking (CXL) methods. The objective of this study was to compare two protocols of epi-off corneal crosslinking-the standard and the accelerated protocol-in terms of efficacy after a one-year follow-up.</p><p><strong>Methods: </strong>41 eyes with progressive keratoconus were treated with corneal crosslinking, either using the accelerated (Acc-CXL) or standard protocol (Std-CXL). The following parameters were monitored: refraction, corneal diopter power on topographic maps (Kmax and Kmin), corneal thickness (CCT), resistance factor (CRF), hysteresis, and the depth of the demarcation line. All measurements were repeated 12 months after the intervention.</p><p><strong>Results: </strong>The progression of keratoconus was halted in 20 eyes using the accelerated method and in 21 eyes using the standard procedure. Both methods resulted in a statistically significant regression of the spherical equivalent, Kmax, and an increase in CCT and CRF, without substantial differences in efficacy. The demarcation line was highlighted on average at a depth of 278.9 ± 31.71 micrometres for the Acc-CXL group and 280.42 ± 47.85 micrometres for the Std-CXL group. It was correlated with the initial topographical values.</p><p><strong>Discussion: </strong>The evaluation of patients revealed no progression of keratoconus following the procedure. Approximately 40% of the cases in the accelerated protocol group and 38.09% of the cases in the standard protocol group have maintained the parameters at a constant level. In comparison, approximately 60% of the cases have shown improvements. An Australian registry revealed that both CXL protocols are safe and effective; however, the standard procedure leads to improved visual acuity, a more significant flattening of the steepest meridian, and a higher chance of an effect greater than one diopter power.</p><p><strong>Conclusions: </strong>Corneal crosslinking (CXL) was effective in halting the progression of keratoconus using both methods. Accelerated CXL is faster and more comfortable for patients, with similar efficiency to standard CXL.</p>\",\"PeriodicalId\":94355,\"journal\":{\"name\":\"Romanian journal of ophthalmology\",\"volume\":\"69 2\",\"pages\":\"175-183\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12277981/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Romanian journal of ophthalmology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22336/rjo.2025.29\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Romanian journal of ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22336/rjo.2025.29","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Standard and accelerated crosslinking protocols in keratoconus - differences and evolution at one year.
Objectives: Keratoconus (KC) is a bilateral, progressive corneal ectasia that involves corneal thinning and a decrease in visual acuity. Stopping the progression of keratoconus can be achieved through various photooxidative crosslinking (CXL) methods. The objective of this study was to compare two protocols of epi-off corneal crosslinking-the standard and the accelerated protocol-in terms of efficacy after a one-year follow-up.
Methods: 41 eyes with progressive keratoconus were treated with corneal crosslinking, either using the accelerated (Acc-CXL) or standard protocol (Std-CXL). The following parameters were monitored: refraction, corneal diopter power on topographic maps (Kmax and Kmin), corneal thickness (CCT), resistance factor (CRF), hysteresis, and the depth of the demarcation line. All measurements were repeated 12 months after the intervention.
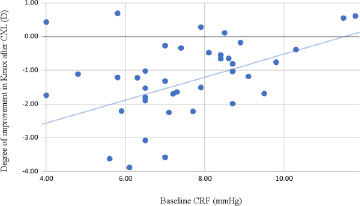
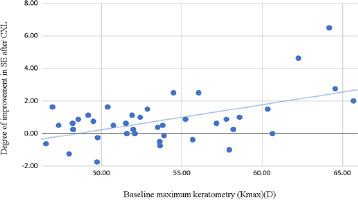
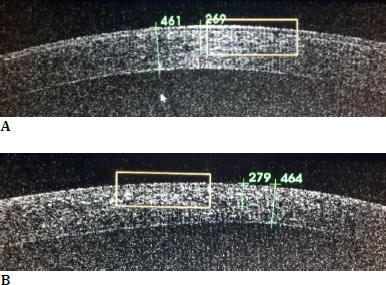
Results: The progression of keratoconus was halted in 20 eyes using the accelerated method and in 21 eyes using the standard procedure. Both methods resulted in a statistically significant regression of the spherical equivalent, Kmax, and an increase in CCT and CRF, without substantial differences in efficacy. The demarcation line was highlighted on average at a depth of 278.9 ± 31.71 micrometres for the Acc-CXL group and 280.42 ± 47.85 micrometres for the Std-CXL group. It was correlated with the initial topographical values.
Discussion: The evaluation of patients revealed no progression of keratoconus following the procedure. Approximately 40% of the cases in the accelerated protocol group and 38.09% of the cases in the standard protocol group have maintained the parameters at a constant level. In comparison, approximately 60% of the cases have shown improvements. An Australian registry revealed that both CXL protocols are safe and effective; however, the standard procedure leads to improved visual acuity, a more significant flattening of the steepest meridian, and a higher chance of an effect greater than one diopter power.
Conclusions: Corneal crosslinking (CXL) was effective in halting the progression of keratoconus using both methods. Accelerated CXL is faster and more comfortable for patients, with similar efficiency to standard CXL.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


