{"title":"头部创伤及休克生命体征患者的预后因素及初步治疗策略。","authors":"Masaki Yasuda, Makoto Ohtake, Taisuke Akimoto, Masayuki Okano, Yuya Imanishi, Takafumi Kawasaki, Jun Suenaga, Katsumi Sakata, Ichiro Takeuchi, Tetsuya Yamamoto","doi":"10.1089/neur.2024.0167","DOIUrl":null,"url":null,"abstract":"<p><p>Head trauma accompanied by circulatory failure is a rare but severe condition, and few reports regarding its prognosis or initial treatment strategies have been published. We aimed to evaluate the prognostic factors and treatment strategies for patients with head trauma and vital signs of shock. We included 415 consecutive patients with head trauma (Abbreviated Injury Scale [AIS] score ≥3) who were transported to our institution from January 2017 to December 2023. These patients were divided into shock and non-shock groups. Data on their background, vital signs at presentation, trunk injury status, surgical intervention, and hematological findings were examined. A retrospective analysis was conducted with the modified Rankin Scale score after 3 months as the primary outcome. The patients' mean age was 53.9 ± 24.4 years, 304 (73.3%) were male, 265 (63.9%) experienced severe trauma (injury severity score ≥16), 124 (29.9%) had multiple trauma (AIS score ≥3 at two or more locations), and 59 (14.2%) had accompanying vital signs of shock (shock index >1). Multivariable analysis revealed that older age (<i>p</i> < 0.0001), a lower Glasgow Coma Scale (GCS) score (<i>p</i> < 0.0001), elevated D-dimer levels (<i>p</i> = 0.0077), and pupillary abnormalities (<i>p</i> = 0.038) were independently associated with a poor prognosis in the non-shock group. In the shock group, older age (<i>p</i> = 0.0037) and neurosurgical intervention (<i>p</i> = 0.012) were independent prognostic factors. In contrast to those in the non-shock group, the GCS score and D-dimer levels were not useful prognostic factors in the shock group. The optimal cut-off age for prognosis was 64 years (area under the receiver operating characteristic curve: 0.752; sensitivity: 0.670, specificity: 0.777). The prognosis was significantly worse in the shock group when neurosurgery was required, suggesting that developing a treatment strategy aimed at more rapidly reducing intracranial pressure is essential, especially for patients under 64 years old with circulatory failure.</p>","PeriodicalId":74300,"journal":{"name":"Neurotrauma reports","volume":"6 1","pages":"336-344"},"PeriodicalIF":1.8000,"publicationDate":"2025-04-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12281107/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic Factors and Initial Treatment Strategies for Patients with Head Trauma and Vital Signs of Shock.\",\"authors\":\"Masaki Yasuda, Makoto Ohtake, Taisuke Akimoto, Masayuki Okano, Yuya Imanishi, Takafumi Kawasaki, Jun Suenaga, Katsumi Sakata, Ichiro Takeuchi, Tetsuya Yamamoto\",\"doi\":\"10.1089/neur.2024.0167\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Head trauma accompanied by circulatory failure is a rare but severe condition, and few reports regarding its prognosis or initial treatment strategies have been published. We aimed to evaluate the prognostic factors and treatment strategies for patients with head trauma and vital signs of shock. We included 415 consecutive patients with head trauma (Abbreviated Injury Scale [AIS] score ≥3) who were transported to our institution from January 2017 to December 2023. These patients were divided into shock and non-shock groups. Data on their background, vital signs at presentation, trunk injury status, surgical intervention, and hematological findings were examined. A retrospective analysis was conducted with the modified Rankin Scale score after 3 months as the primary outcome. The patients' mean age was 53.9 ± 24.4 years, 304 (73.3%) were male, 265 (63.9%) experienced severe trauma (injury severity score ≥16), 124 (29.9%) had multiple trauma (AIS score ≥3 at two or more locations), and 59 (14.2%) had accompanying vital signs of shock (shock index >1). Multivariable analysis revealed that older age (<i>p</i> < 0.0001), a lower Glasgow Coma Scale (GCS) score (<i>p</i> < 0.0001), elevated D-dimer levels (<i>p</i> = 0.0077), and pupillary abnormalities (<i>p</i> = 0.038) were independently associated with a poor prognosis in the non-shock group. In the shock group, older age (<i>p</i> = 0.0037) and neurosurgical intervention (<i>p</i> = 0.012) were independent prognostic factors. In contrast to those in the non-shock group, the GCS score and D-dimer levels were not useful prognostic factors in the shock group. The optimal cut-off age for prognosis was 64 years (area under the receiver operating characteristic curve: 0.752; sensitivity: 0.670, specificity: 0.777). The prognosis was significantly worse in the shock group when neurosurgery was required, suggesting that developing a treatment strategy aimed at more rapidly reducing intracranial pressure is essential, especially for patients under 64 years old with circulatory failure.</p>\",\"PeriodicalId\":74300,\"journal\":{\"name\":\"Neurotrauma reports\",\"volume\":\"6 1\",\"pages\":\"336-344\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-04-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12281107/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurotrauma reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1089/neur.2024.0167\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurotrauma reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/neur.2024.0167","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Prognostic Factors and Initial Treatment Strategies for Patients with Head Trauma and Vital Signs of Shock.
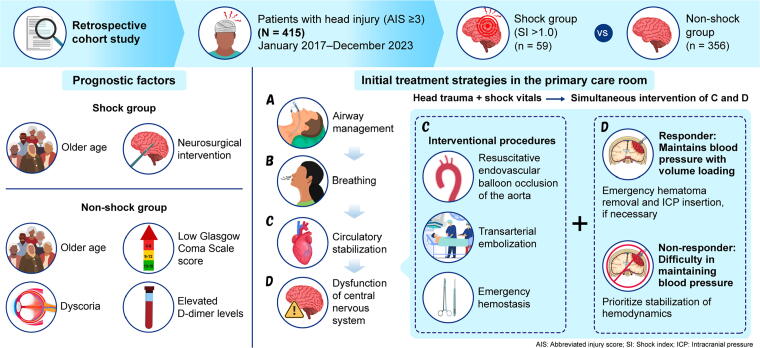
Head trauma accompanied by circulatory failure is a rare but severe condition, and few reports regarding its prognosis or initial treatment strategies have been published. We aimed to evaluate the prognostic factors and treatment strategies for patients with head trauma and vital signs of shock. We included 415 consecutive patients with head trauma (Abbreviated Injury Scale [AIS] score ≥3) who were transported to our institution from January 2017 to December 2023. These patients were divided into shock and non-shock groups. Data on their background, vital signs at presentation, trunk injury status, surgical intervention, and hematological findings were examined. A retrospective analysis was conducted with the modified Rankin Scale score after 3 months as the primary outcome. The patients' mean age was 53.9 ± 24.4 years, 304 (73.3%) were male, 265 (63.9%) experienced severe trauma (injury severity score ≥16), 124 (29.9%) had multiple trauma (AIS score ≥3 at two or more locations), and 59 (14.2%) had accompanying vital signs of shock (shock index >1). Multivariable analysis revealed that older age (p < 0.0001), a lower Glasgow Coma Scale (GCS) score (p < 0.0001), elevated D-dimer levels (p = 0.0077), and pupillary abnormalities (p = 0.038) were independently associated with a poor prognosis in the non-shock group. In the shock group, older age (p = 0.0037) and neurosurgical intervention (p = 0.012) were independent prognostic factors. In contrast to those in the non-shock group, the GCS score and D-dimer levels were not useful prognostic factors in the shock group. The optimal cut-off age for prognosis was 64 years (area under the receiver operating characteristic curve: 0.752; sensitivity: 0.670, specificity: 0.777). The prognosis was significantly worse in the shock group when neurosurgery was required, suggesting that developing a treatment strategy aimed at more rapidly reducing intracranial pressure is essential, especially for patients under 64 years old with circulatory failure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


