{"title":"无骨水泥双极半关节置换术与股骨近端钉抗旋转治疗不稳定转子间骨折的疗效比较:荟萃分析。","authors":"Ahmed Mohamed Yousif Mohamed, Monzir Salih, Mugahid Mohamed, Ayman E Abbas, Maysara Elsiddig, Moaz Osama Omar, Mazin Abdelsalam, Basil Elhag, Nujud Mohamed, Souzan Hassan Eisa Ahmed, Samah Ahmed, Duaa Mohamed, Deena Omar","doi":"10.5312/wjo.v16.i7.107950","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Unstable intertrochanteric fractures in elderly patients require effective surgical management, with both cementless bipolar hemiarthroplasty (CBHA) and proximal femoral nail anti-rotation (PFNA) being valid treatment options to reduce morbidity and mortality.</p><p><strong>Aim: </strong>To evaluate and compare the outcomes of CBHA and PFNA in treatment of unstable intertrochanteric fractures.</p><p><strong>Methods: </strong>A comprehensive search was conducted to identify relevant studies discussing the outcomes of using both CBH and PFNA in treatment of unstable intertrochanteric fractures. Studies published up to January 1, 2025 were searched across multiple databases, including PubMed, EMBASE, Scopus, Web of Science, Cochrane Library, and Google Scholar. Full texts of the selected articles were retrieved, reviewed, and independently assessed by the investigators. Discrepancies were resolved by consensus, with any remaining disagreements being arbitrated by a third author.</p><p><strong>Results: </strong>This meta-analysis included three studies, all of which were retrospective, involving a total of 240 patients. The follow-up period for participants was at least 12 months. CBHA was associated with significantly higher blood loss compared to PFNA [mean differences (MD): 129.14, 95%CI (52.51, 205.77), <i>P</i> = 0.001], though heterogeneity was high (<i>I</i>² = 97%). Operative time showed no significant difference initially [MD: 6.10, 95%CI (-13.34, 25.54), <i>P</i> = 0.54], but after excluding one study, BHA had longer operative times [MD: 21.51, 95%CI (18.60, 24.41), <i>P</i> < 0.00001]. Hospital stay and Harris scores showed no significant differences between groups. CBHA facilitated faster progression to weight-bearing [MD: -11.92, 95%CI (-22.46, -1.39), <i>P</i> = 0.03] and a lower incidence of prosthetic loosening [risk ratio: 0.21, 95%CI (0.05, 0.92), <i>P</i> = 0.04]. Refracture and thrombus formation rates were comparable between the two groups.</p><p><strong>Conclusion: </strong>CBHA offers shorter weight-bearing duration and reduced prosthetic loosening but incurs greater blood loss and longer operative times compared to PFNA. Both techniques show comparable functional recovery, hospital stay, refracture, and thrombus risks. Clinical choice should prioritize early mobilization or surgical minimalism, guided by patient needs. Further prospective studies are warranted.</p>","PeriodicalId":47843,"journal":{"name":"World Journal of Orthopedics","volume":"16 7","pages":"107950"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12278281/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparative efficacy of cementless bipolar hemiarthroplasty and proximal femoral nail anti-rotation in unstable intertrochanteric fractures: A meta-analysis.\",\"authors\":\"Ahmed Mohamed Yousif Mohamed, Monzir Salih, Mugahid Mohamed, Ayman E Abbas, Maysara Elsiddig, Moaz Osama Omar, Mazin Abdelsalam, Basil Elhag, Nujud Mohamed, Souzan Hassan Eisa Ahmed, Samah Ahmed, Duaa Mohamed, Deena Omar\",\"doi\":\"10.5312/wjo.v16.i7.107950\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Unstable intertrochanteric fractures in elderly patients require effective surgical management, with both cementless bipolar hemiarthroplasty (CBHA) and proximal femoral nail anti-rotation (PFNA) being valid treatment options to reduce morbidity and mortality.</p><p><strong>Aim: </strong>To evaluate and compare the outcomes of CBHA and PFNA in treatment of unstable intertrochanteric fractures.</p><p><strong>Methods: </strong>A comprehensive search was conducted to identify relevant studies discussing the outcomes of using both CBH and PFNA in treatment of unstable intertrochanteric fractures. Studies published up to January 1, 2025 were searched across multiple databases, including PubMed, EMBASE, Scopus, Web of Science, Cochrane Library, and Google Scholar. Full texts of the selected articles were retrieved, reviewed, and independently assessed by the investigators. Discrepancies were resolved by consensus, with any remaining disagreements being arbitrated by a third author.</p><p><strong>Results: </strong>This meta-analysis included three studies, all of which were retrospective, involving a total of 240 patients. The follow-up period for participants was at least 12 months. CBHA was associated with significantly higher blood loss compared to PFNA [mean differences (MD): 129.14, 95%CI (52.51, 205.77), <i>P</i> = 0.001], though heterogeneity was high (<i>I</i>² = 97%). Operative time showed no significant difference initially [MD: 6.10, 95%CI (-13.34, 25.54), <i>P</i> = 0.54], but after excluding one study, BHA had longer operative times [MD: 21.51, 95%CI (18.60, 24.41), <i>P</i> < 0.00001]. Hospital stay and Harris scores showed no significant differences between groups. CBHA facilitated faster progression to weight-bearing [MD: -11.92, 95%CI (-22.46, -1.39), <i>P</i> = 0.03] and a lower incidence of prosthetic loosening [risk ratio: 0.21, 95%CI (0.05, 0.92), <i>P</i> = 0.04]. Refracture and thrombus formation rates were comparable between the two groups.</p><p><strong>Conclusion: </strong>CBHA offers shorter weight-bearing duration and reduced prosthetic loosening but incurs greater blood loss and longer operative times compared to PFNA. Both techniques show comparable functional recovery, hospital stay, refracture, and thrombus risks. Clinical choice should prioritize early mobilization or surgical minimalism, guided by patient needs. Further prospective studies are warranted.</p>\",\"PeriodicalId\":47843,\"journal\":{\"name\":\"World Journal of Orthopedics\",\"volume\":\"16 7\",\"pages\":\"107950\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12278281/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Orthopedics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5312/wjo.v16.i7.107950\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5312/wjo.v16.i7.107950","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
背景:老年患者不稳定转子间骨折需要有效的手术治疗,无骨水泥双极半关节置换术(CBHA)和股骨近端钉抗旋转(PFNA)是降低发病率和死亡率的有效治疗选择。目的:评价和比较CBHA与PFNA治疗不稳定转子间骨折的疗效。方法:综合检索探讨CBH和PFNA治疗不稳定转子间骨折疗效的相关研究。截至2025年1月1日发表的研究在多个数据库中进行了检索,包括PubMed, EMBASE, Scopus, Web of Science, Cochrane Library和谷歌Scholar。所选文章的全文被检索、审查,并由研究者独立评估。差异以协商一致方式解决,其余分歧由第三作者仲裁。结果:本荟萃分析包括三项研究,均为回顾性研究,共涉及240例患者。参与者的随访期至少为12个月。与PFNA相比,CBHA显着增加了出血量[平均差异(MD): 129.14, 95%CI (52.51, 205.77), P = 0.001],尽管异质性很高(I²= 97%)。初始手术时间差异无统计学意义[MD: 6.10, 95%CI (-13.34, 25.54), P = 0.54],但排除1项研究后,BHA手术时间延长[MD: 21.51, 95%CI (18.60, 24.41), P < 0.00001]。住院时间和哈里斯评分在两组间无显著差异。CBHA促进了更快的负重进展[MD: -11.92, 95%CI (-22.46, -1.39), P = 0.03]和更低的假体松动发生率[风险比:0.21,95%CI (0.05, 0.92), P = 0.04]。两组之间的再破裂和血栓形成率具有可比性。结论:与PFNA相比,CBHA具有更短的负重时间和更少的假体松动,但会导致更大的失血量和更长的手术时间。两种技术显示出相当的功能恢复、住院时间、再骨折和血栓风险。临床选择应优先考虑早期活动或手术微创,以患者的需要为指导。进一步的前瞻性研究是必要的。
Comparative efficacy of cementless bipolar hemiarthroplasty and proximal femoral nail anti-rotation in unstable intertrochanteric fractures: A meta-analysis.
Background: Unstable intertrochanteric fractures in elderly patients require effective surgical management, with both cementless bipolar hemiarthroplasty (CBHA) and proximal femoral nail anti-rotation (PFNA) being valid treatment options to reduce morbidity and mortality.
Aim: To evaluate and compare the outcomes of CBHA and PFNA in treatment of unstable intertrochanteric fractures.
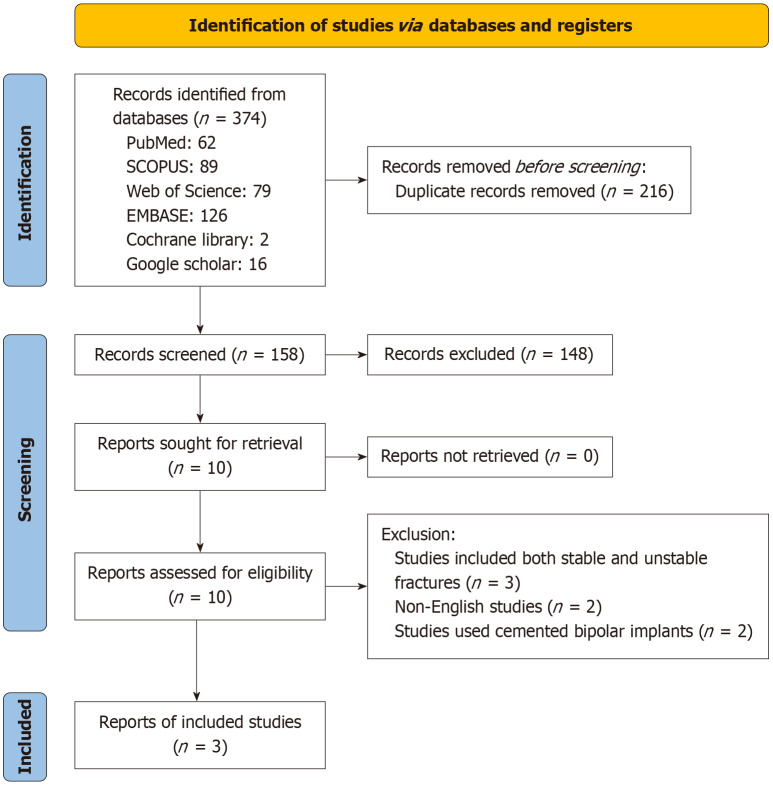
Methods: A comprehensive search was conducted to identify relevant studies discussing the outcomes of using both CBH and PFNA in treatment of unstable intertrochanteric fractures. Studies published up to January 1, 2025 were searched across multiple databases, including PubMed, EMBASE, Scopus, Web of Science, Cochrane Library, and Google Scholar. Full texts of the selected articles were retrieved, reviewed, and independently assessed by the investigators. Discrepancies were resolved by consensus, with any remaining disagreements being arbitrated by a third author.
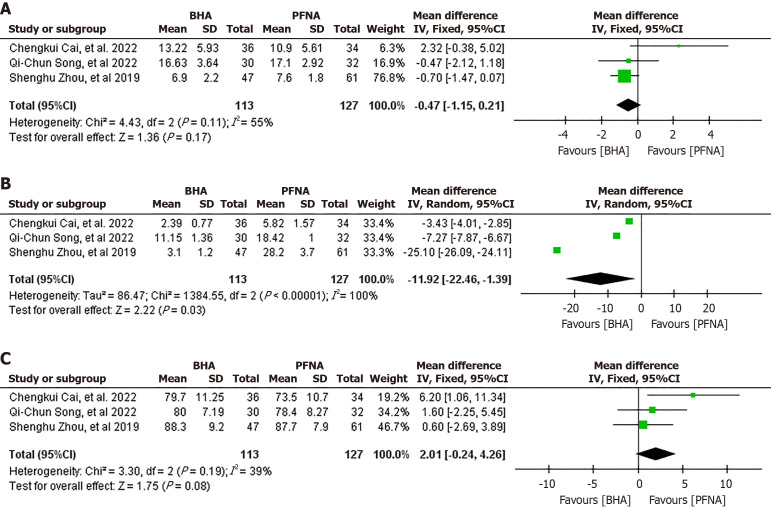
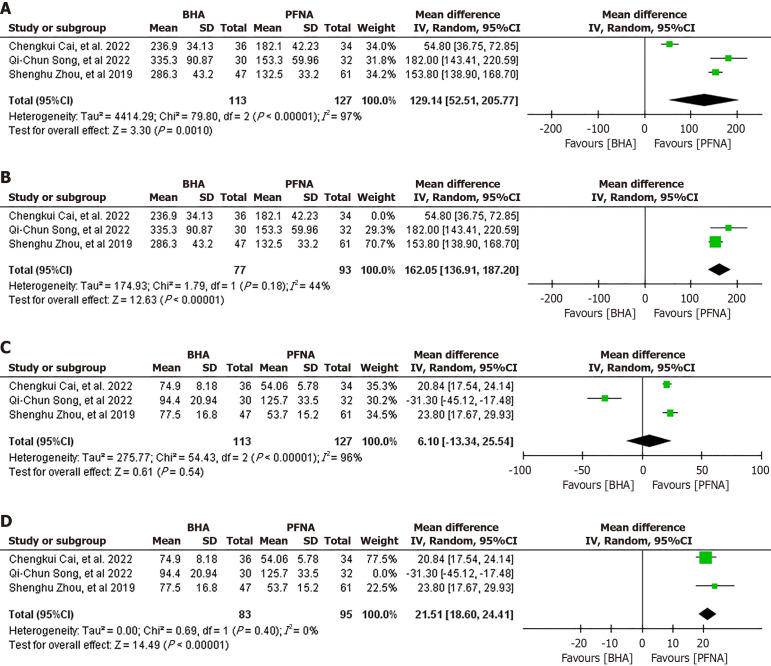
Results: This meta-analysis included three studies, all of which were retrospective, involving a total of 240 patients. The follow-up period for participants was at least 12 months. CBHA was associated with significantly higher blood loss compared to PFNA [mean differences (MD): 129.14, 95%CI (52.51, 205.77), P = 0.001], though heterogeneity was high (I² = 97%). Operative time showed no significant difference initially [MD: 6.10, 95%CI (-13.34, 25.54), P = 0.54], but after excluding one study, BHA had longer operative times [MD: 21.51, 95%CI (18.60, 24.41), P < 0.00001]. Hospital stay and Harris scores showed no significant differences between groups. CBHA facilitated faster progression to weight-bearing [MD: -11.92, 95%CI (-22.46, -1.39), P = 0.03] and a lower incidence of prosthetic loosening [risk ratio: 0.21, 95%CI (0.05, 0.92), P = 0.04]. Refracture and thrombus formation rates were comparable between the two groups.
Conclusion: CBHA offers shorter weight-bearing duration and reduced prosthetic loosening but incurs greater blood loss and longer operative times compared to PFNA. Both techniques show comparable functional recovery, hospital stay, refracture, and thrombus risks. Clinical choice should prioritize early mobilization or surgical minimalism, guided by patient needs. Further prospective studies are warranted.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


