Qiong-Ya Guo, Wei Zhang, Lin Fu, Shan-Shan Hu, Lin Li
{"title":"局部晚期直肠癌新辅助放化疗治疗反应的nomogram模型的预测价值。","authors":"Qiong-Ya Guo, Wei Zhang, Lin Fu, Shan-Shan Hu, Lin Li","doi":"10.4251/wjgo.v17.i7.105403","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Locally advanced rectal cancer (LARC) carries a substantial risk of recurrence, prompting the use of neoadjuvant chemoradiotherapy (nCRT) to improve tumor resectability and long-term outcomes. However, individual treatment responses vary considerably, highlighting the need for robust predictive tools to guide clinical decision-making.</p><p><strong>Aim: </strong>To develop a nomogram model integrating clinical characteristics and biomarkers to predict the likelihood of poor response to nCRT in LARC.</p><p><strong>Methods: </strong>A retrospective analysis was performed on 178 patients with stage II-III LARC treated from January 2021 to December 2023. All patients underwent standardized nCRT followed by total mesorectal excision. Clinical data, inflammatory markers [C-reactive protein (CRP), interleukin-6 (IL-6), tumor necrosis factor-alpha], and tumor markers [carcinoembryonic antigen (CEA), carbohydrate antigen 19-9] were collected. Logistic regression was used to identify independent predictors of poor nCRT response. A nomogram was constructed using significant predictors and validated <i>via</i> concordance index (C-index), receiver operating characteristic curve, calibration plot, and decision curve analysis (DCA).</p><p><strong>Results: </strong>A total of 178 patients were enrolled, with 36 (20.2%) achieving a good response and 142 (79.8%) exhibiting a poor response to nCRT. Baseline factors, including age and comorbidities, showed no significant differences. However, poor responders more frequently had lymph node metastasis, advanced tumor node metastasis/T stage, larger tumor diameter, and elevated CRP, IL-6, and CEA levels. Logistic regression confirmed CRP, IL-6, and CEA as independent predictors of poor response. The nomogram demonstrated high accuracy (area under the curve = 0.928), good calibration (Hosmer-Lemeshow <i>P</i> = 0.928), and a sensitivity of 88.1% with 82.6% specificity. Internal validation <i>via</i> bootstrap resampling (<i>n</i> = 1000) yielded an adjusted C-index of 0.716, and DCA confirmed substantial clinical utility.</p><p><strong>Conclusion: </strong>A nomogram incorporating serum CRP, IL-6, and CEA accurately predicts poor nCRT response in patients with LARC. This model provides a valuable framework for individualized treatment planning, potentially improving clinical outcomes.</p>","PeriodicalId":23762,"journal":{"name":"World Journal of Gastrointestinal Oncology","volume":"17 7","pages":"105403"},"PeriodicalIF":2.5000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12278235/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predictive value of a nomogram model for treatment response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer.\",\"authors\":\"Qiong-Ya Guo, Wei Zhang, Lin Fu, Shan-Shan Hu, Lin Li\",\"doi\":\"10.4251/wjgo.v17.i7.105403\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Locally advanced rectal cancer (LARC) carries a substantial risk of recurrence, prompting the use of neoadjuvant chemoradiotherapy (nCRT) to improve tumor resectability and long-term outcomes. However, individual treatment responses vary considerably, highlighting the need for robust predictive tools to guide clinical decision-making.</p><p><strong>Aim: </strong>To develop a nomogram model integrating clinical characteristics and biomarkers to predict the likelihood of poor response to nCRT in LARC.</p><p><strong>Methods: </strong>A retrospective analysis was performed on 178 patients with stage II-III LARC treated from January 2021 to December 2023. All patients underwent standardized nCRT followed by total mesorectal excision. Clinical data, inflammatory markers [C-reactive protein (CRP), interleukin-6 (IL-6), tumor necrosis factor-alpha], and tumor markers [carcinoembryonic antigen (CEA), carbohydrate antigen 19-9] were collected. Logistic regression was used to identify independent predictors of poor nCRT response. A nomogram was constructed using significant predictors and validated <i>via</i> concordance index (C-index), receiver operating characteristic curve, calibration plot, and decision curve analysis (DCA).</p><p><strong>Results: </strong>A total of 178 patients were enrolled, with 36 (20.2%) achieving a good response and 142 (79.8%) exhibiting a poor response to nCRT. Baseline factors, including age and comorbidities, showed no significant differences. However, poor responders more frequently had lymph node metastasis, advanced tumor node metastasis/T stage, larger tumor diameter, and elevated CRP, IL-6, and CEA levels. Logistic regression confirmed CRP, IL-6, and CEA as independent predictors of poor response. The nomogram demonstrated high accuracy (area under the curve = 0.928), good calibration (Hosmer-Lemeshow <i>P</i> = 0.928), and a sensitivity of 88.1% with 82.6% specificity. Internal validation <i>via</i> bootstrap resampling (<i>n</i> = 1000) yielded an adjusted C-index of 0.716, and DCA confirmed substantial clinical utility.</p><p><strong>Conclusion: </strong>A nomogram incorporating serum CRP, IL-6, and CEA accurately predicts poor nCRT response in patients with LARC. This model provides a valuable framework for individualized treatment planning, potentially improving clinical outcomes.</p>\",\"PeriodicalId\":23762,\"journal\":{\"name\":\"World Journal of Gastrointestinal Oncology\",\"volume\":\"17 7\",\"pages\":\"105403\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12278235/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastrointestinal Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4251/wjgo.v17.i7.105403\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4251/wjgo.v17.i7.105403","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:局部晚期直肠癌(LARC)具有很大的复发风险,促使人们使用新辅助放化疗(nCRT)来改善肿瘤的可切除性和长期预后。然而,个体治疗反应差异很大,强调需要强大的预测工具来指导临床决策。目的:建立一种结合临床特征和生物标志物的nomogram模型来预测LARC患者对nCRT不良反应的可能性。方法:回顾性分析2021年1月至2023年12月期间接受治疗的178例II-III期LARC患者。所有患者都接受了标准化的nCRT,随后进行了全肠系膜切除术。收集临床资料、炎症标志物[c反应蛋白(CRP)、白细胞介素-6 (IL-6)、肿瘤坏死因子- α]和肿瘤标志物[癌胚抗原(CEA)、碳水化合物抗原19-9]。使用逻辑回归来确定nCRT不良反应的独立预测因素。采用显著性预测因子构建nomogram,并通过一致性指数(C-index)、受试者工作特征曲线、校准图和决策曲线分析(DCA)进行验证。结果:共纳入178例患者,其中36例(20.2%)获得良好反应,142例(79.8%)表现出不良反应。基线因素,包括年龄和合并症,没有显着差异。然而,不良应答者更多出现淋巴结转移、晚期肿瘤淋巴结转移/T期、肿瘤直径较大、CRP、IL-6和CEA水平升高。Logistic回归证实CRP、IL-6和CEA是不良反应的独立预测因子。该方法准确度高(曲线下面积= 0.928),标度好(Hosmer-Lemeshow P = 0.928),灵敏度为88.1%,特异度为82.6%。通过bootstrap重新采样(n = 1000)进行内部验证,调整后的c指数为0.716,DCA证实了大量的临床应用。结论:结合血清CRP、IL-6和CEA的nomogram可准确预测LARC患者nCRT不良反应。该模型为个性化治疗计划提供了一个有价值的框架,有可能改善临床结果。
Predictive value of a nomogram model for treatment response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer.
Background: Locally advanced rectal cancer (LARC) carries a substantial risk of recurrence, prompting the use of neoadjuvant chemoradiotherapy (nCRT) to improve tumor resectability and long-term outcomes. However, individual treatment responses vary considerably, highlighting the need for robust predictive tools to guide clinical decision-making.
Aim: To develop a nomogram model integrating clinical characteristics and biomarkers to predict the likelihood of poor response to nCRT in LARC.
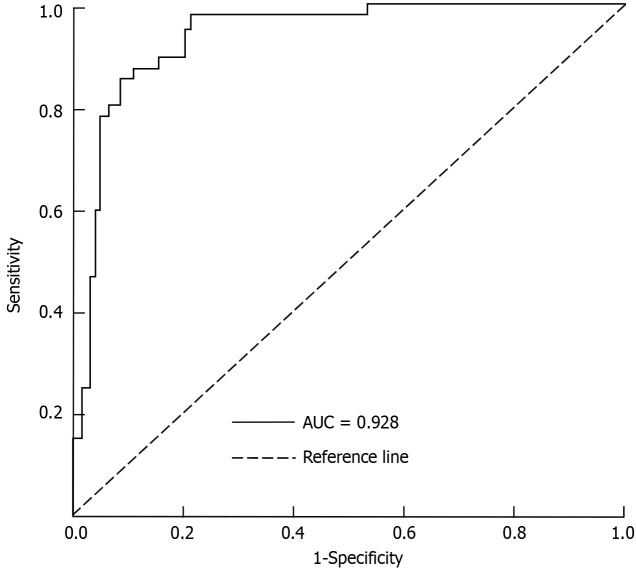
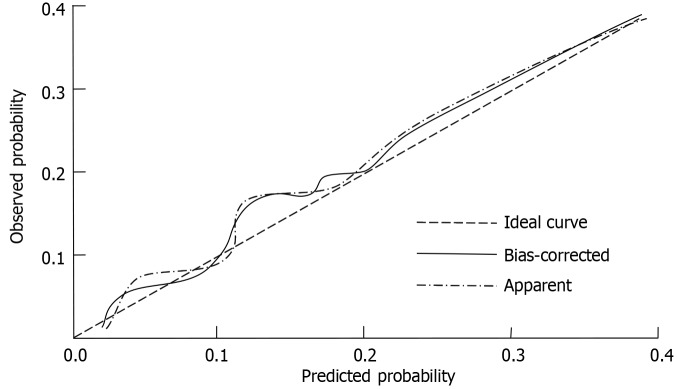
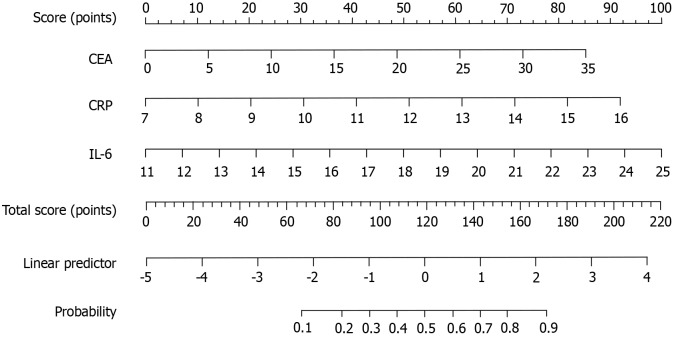
Methods: A retrospective analysis was performed on 178 patients with stage II-III LARC treated from January 2021 to December 2023. All patients underwent standardized nCRT followed by total mesorectal excision. Clinical data, inflammatory markers [C-reactive protein (CRP), interleukin-6 (IL-6), tumor necrosis factor-alpha], and tumor markers [carcinoembryonic antigen (CEA), carbohydrate antigen 19-9] were collected. Logistic regression was used to identify independent predictors of poor nCRT response. A nomogram was constructed using significant predictors and validated via concordance index (C-index), receiver operating characteristic curve, calibration plot, and decision curve analysis (DCA).
Results: A total of 178 patients were enrolled, with 36 (20.2%) achieving a good response and 142 (79.8%) exhibiting a poor response to nCRT. Baseline factors, including age and comorbidities, showed no significant differences. However, poor responders more frequently had lymph node metastasis, advanced tumor node metastasis/T stage, larger tumor diameter, and elevated CRP, IL-6, and CEA levels. Logistic regression confirmed CRP, IL-6, and CEA as independent predictors of poor response. The nomogram demonstrated high accuracy (area under the curve = 0.928), good calibration (Hosmer-Lemeshow P = 0.928), and a sensitivity of 88.1% with 82.6% specificity. Internal validation via bootstrap resampling (n = 1000) yielded an adjusted C-index of 0.716, and DCA confirmed substantial clinical utility.
Conclusion: A nomogram incorporating serum CRP, IL-6, and CEA accurately predicts poor nCRT response in patients with LARC. This model provides a valuable framework for individualized treatment planning, potentially improving clinical outcomes.
期刊介绍:
The World Journal of Gastrointestinal Oncology (WJGO) is a leading academic journal devoted to reporting the latest, cutting-edge research progress and findings of basic research and clinical practice in the field of gastrointestinal oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


