{"title":"糖尿病患者胱抑素C、肌酐和血清GDF-15的eGFR差异与不良结局的关系","authors":"Tomohito Gohda, Nozomu Kamei, Marenao Tanaka, Masato Furuhashi, Tatsuya Sato, Mitsunobu Kubota, Michiyoshi Sanuki, Takeo Koshida, Shinji Hagiwara, Yusuke Suzuki, Maki Murakoshi","doi":"10.1002/jcsm.70011","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Protein catabolism and chronic inflammation drive sarcopenia and frailty in individuals with diabetes mellitus and chronic kidney disease (CKD). The difference between estimated glomerular filtration rates derived from cystatin C and creatinine (eGFRcys and eGFRcr, respectively), termed eGFRdiff, along with growth differentiation factor-15 (GDF-15) levels, have emerged as markers of metabolic and inflammatory dysregulation. Lower eGFRdiff and elevated GDF-15 levels are associated with sarcopenia, frailty, CKD progression and mortality. However, their interplay and respective impacts on CKD progression and mortality remain unclear.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A total of 638 Japanese individuals with diabetes mellitus were stratified into tertiles based on eGFRdiff. Serum GDF-15 levels were measured using enzyme-linked immunosorbent assays. The relationships between eGFRdiff and GDF-15 were assessed using Spearman's correlation coefficients. Multivariate ordered logistic regression was used to evaluate the association between eGFRdiff and GDF-15 tertiles, with GDF-15 as the dependent variable and eGFRdiff as the independent variable, adjusting for covariates including age, sex, urinary albumin-to-creatinine ratio (UACR) and eGFRcr or eGFRcys. Cox proportional hazards models with restricted cubic splines were used to examine associations between eGFRdiff and GDF-15 (independent variables) with CKD progression (≥ 30% decline in eGFRcr from baseline) and mortality (dependent variables). These models were adjusted for age, sex, glycated haemoglobin, UACR and eGFRcr.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The median age was 65 years (interquartile range: 58–73), and 53.9% of participants were male. Over median follow-up periods of 5.3 years for CKD progression and 5.4 years for mortality, 75 participants (11.8%) experienced CKD progression and 44 (6.9%) died. GDF-15 levels inversely correlated with eGFRdiff (<i>r</i> = −0.35, <i>p</i> < 0.001). Higher eGFRdiff values were associated with lower odds of being in a higher GDF-15 tertile (odds ratio 0.86; 95% confidence interval [CI]: 0.76–0.97; <i>p</i> = 0.01). Both lower eGFRdiff and higher GDF-15 levels were independently associated with adverse outcomes: CKD progression (GDF-15, hazard ratio [HR] 1.36, 95% CI: 1.02–1.81, <i>p</i> < 0.05; eGFRdiff, HR 0.67, 95% CI: 0.58–0.78, <i>p</i> < 0.0001) and mortality (GDF-15, HR 2.35, 95% CI: 1.63–3.41, <i>p</i> < 0.0001; eGFRdiff: 0.80, 95% CI: 0.65–0.99, <i>p</i> < 0.05).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Both eGFRdiff and GDF-15 were independently associated with adverse outcomes in individuals with diabetes mellitus. GDF-15 showed a stronger association with mortality, whereas eGFRdiff was more strongly linked to CKD progression. These findings underscore the potential utility of these markers in risk stratification for diabetes-related complications and may guide individualized interventions in clinical practice.</p>\n </section>\n </div>","PeriodicalId":48911,"journal":{"name":"Journal of Cachexia Sarcopenia and Muscle","volume":"16 4","pages":""},"PeriodicalIF":9.1000,"publicationDate":"2025-07-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jcsm.70011","citationCount":"0","resultStr":"{\"title\":\"Association of Difference Between eGFR From Cystatin C and Creatinine and Serum GDF-15 With Adverse Outcomes in Diabetes Mellitus\",\"authors\":\"Tomohito Gohda, Nozomu Kamei, Marenao Tanaka, Masato Furuhashi, Tatsuya Sato, Mitsunobu Kubota, Michiyoshi Sanuki, Takeo Koshida, Shinji Hagiwara, Yusuke Suzuki, Maki Murakoshi\",\"doi\":\"10.1002/jcsm.70011\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Protein catabolism and chronic inflammation drive sarcopenia and frailty in individuals with diabetes mellitus and chronic kidney disease (CKD). The difference between estimated glomerular filtration rates derived from cystatin C and creatinine (eGFRcys and eGFRcr, respectively), termed eGFRdiff, along with growth differentiation factor-15 (GDF-15) levels, have emerged as markers of metabolic and inflammatory dysregulation. Lower eGFRdiff and elevated GDF-15 levels are associated with sarcopenia, frailty, CKD progression and mortality. However, their interplay and respective impacts on CKD progression and mortality remain unclear.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>A total of 638 Japanese individuals with diabetes mellitus were stratified into tertiles based on eGFRdiff. Serum GDF-15 levels were measured using enzyme-linked immunosorbent assays. The relationships between eGFRdiff and GDF-15 were assessed using Spearman's correlation coefficients. Multivariate ordered logistic regression was used to evaluate the association between eGFRdiff and GDF-15 tertiles, with GDF-15 as the dependent variable and eGFRdiff as the independent variable, adjusting for covariates including age, sex, urinary albumin-to-creatinine ratio (UACR) and eGFRcr or eGFRcys. Cox proportional hazards models with restricted cubic splines were used to examine associations between eGFRdiff and GDF-15 (independent variables) with CKD progression (≥ 30% decline in eGFRcr from baseline) and mortality (dependent variables). These models were adjusted for age, sex, glycated haemoglobin, UACR and eGFRcr.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The median age was 65 years (interquartile range: 58–73), and 53.9% of participants were male. Over median follow-up periods of 5.3 years for CKD progression and 5.4 years for mortality, 75 participants (11.8%) experienced CKD progression and 44 (6.9%) died. GDF-15 levels inversely correlated with eGFRdiff (<i>r</i> = −0.35, <i>p</i> < 0.001). Higher eGFRdiff values were associated with lower odds of being in a higher GDF-15 tertile (odds ratio 0.86; 95% confidence interval [CI]: 0.76–0.97; <i>p</i> = 0.01). Both lower eGFRdiff and higher GDF-15 levels were independently associated with adverse outcomes: CKD progression (GDF-15, hazard ratio [HR] 1.36, 95% CI: 1.02–1.81, <i>p</i> < 0.05; eGFRdiff, HR 0.67, 95% CI: 0.58–0.78, <i>p</i> < 0.0001) and mortality (GDF-15, HR 2.35, 95% CI: 1.63–3.41, <i>p</i> < 0.0001; eGFRdiff: 0.80, 95% CI: 0.65–0.99, <i>p</i> < 0.05).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Both eGFRdiff and GDF-15 were independently associated with adverse outcomes in individuals with diabetes mellitus. GDF-15 showed a stronger association with mortality, whereas eGFRdiff was more strongly linked to CKD progression. These findings underscore the potential utility of these markers in risk stratification for diabetes-related complications and may guide individualized interventions in clinical practice.</p>\\n </section>\\n </div>\",\"PeriodicalId\":48911,\"journal\":{\"name\":\"Journal of Cachexia Sarcopenia and Muscle\",\"volume\":\"16 4\",\"pages\":\"\"},\"PeriodicalIF\":9.1000,\"publicationDate\":\"2025-07-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jcsm.70011\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cachexia Sarcopenia and Muscle\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jcsm.70011\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cachexia Sarcopenia and Muscle","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jcsm.70011","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
在糖尿病和慢性肾脏疾病(CKD)患者中,蛋白质分解代谢和慢性炎症导致肌肉减少和虚弱。由胱抑素C和肌酐(分别为eGFRcys和eGFRcr)估算的肾小球滤过率之间的差异,称为eGFRdiff,以及生长分化因子-15 (GDF-15)水平,已成为代谢和炎症失调的标志。eGFRdiff降低和GDF-15水平升高与肌肉减少症、虚弱、CKD进展和死亡率相关。然而,它们对CKD进展和死亡率的相互作用和各自的影响尚不清楚。方法采用eGFRdiff对638例日本糖尿病患者进行分组。采用酶联免疫吸附法测定血清GDF-15水平。使用Spearman相关系数评估eGFRdiff与GDF-15之间的关系。以GDF-15为因变量,eGFRdiff为自变量,采用多变量有序逻辑回归评估eGFRdiff与GDF-15分位数之间的相关性,调整协变量包括年龄、性别、尿白蛋白与肌酐比(UACR)和eGFRcr或eGFRcys。使用限制性三次样条的Cox比例风险模型来检查eGFRdiff和GDF-15(自变量)与CKD进展(eGFRcr较基线下降≥30%)和死亡率(因变量)之间的关系。这些模型根据年龄、性别、糖化血红蛋白、UACR和eGFRcr进行了调整。结果中位年龄为65岁(四分位数范围为58 ~ 73岁),男性占53.9%。在CKD进展的中位随访期5.3年,死亡率的中位随访期5.4年,75名参与者(11.8%)经历CKD进展,44名参与者(6.9%)死亡。GDF-15水平与eGFRdiff呈负相关(r = - 0.35, p < 0.001)。较高的eGFRdiff值与较高GDF-15分位数的几率较低相关(优势比0.86;95%置信区间[CI]: 0.76-0.97;p = 0.01)。较低的eGFRdiff和较高的GDF-15水平均与不良结局独立相关:CKD进展(GDF-15,风险比[HR] 1.36, 95% CI: 1.02-1.81, p < 0.05;eGFRdiff, HR 0.67, 95% CI: 0.58-0.78, p < 0.0001)和死亡率(GDF-15, HR 2.35, 95% CI: 1.63-3.41, p < 0.0001;eGFRdiff: 0.80, 95% CI: 0.65-0.99, p < 0.05)。结论:eGFRdiff和GDF-15与糖尿病患者的不良结局独立相关。GDF-15与死亡率的相关性更强,而eGFRdiff与CKD进展的相关性更强。这些发现强调了这些标志物在糖尿病相关并发症风险分层中的潜在效用,并可能指导临床实践中的个体化干预。
Association of Difference Between eGFR From Cystatin C and Creatinine and Serum GDF-15 With Adverse Outcomes in Diabetes Mellitus
Background
Protein catabolism and chronic inflammation drive sarcopenia and frailty in individuals with diabetes mellitus and chronic kidney disease (CKD). The difference between estimated glomerular filtration rates derived from cystatin C and creatinine (eGFRcys and eGFRcr, respectively), termed eGFRdiff, along with growth differentiation factor-15 (GDF-15) levels, have emerged as markers of metabolic and inflammatory dysregulation. Lower eGFRdiff and elevated GDF-15 levels are associated with sarcopenia, frailty, CKD progression and mortality. However, their interplay and respective impacts on CKD progression and mortality remain unclear.
Methods
A total of 638 Japanese individuals with diabetes mellitus were stratified into tertiles based on eGFRdiff. Serum GDF-15 levels were measured using enzyme-linked immunosorbent assays. The relationships between eGFRdiff and GDF-15 were assessed using Spearman's correlation coefficients. Multivariate ordered logistic regression was used to evaluate the association between eGFRdiff and GDF-15 tertiles, with GDF-15 as the dependent variable and eGFRdiff as the independent variable, adjusting for covariates including age, sex, urinary albumin-to-creatinine ratio (UACR) and eGFRcr or eGFRcys. Cox proportional hazards models with restricted cubic splines were used to examine associations between eGFRdiff and GDF-15 (independent variables) with CKD progression (≥ 30% decline in eGFRcr from baseline) and mortality (dependent variables). These models were adjusted for age, sex, glycated haemoglobin, UACR and eGFRcr.
Results
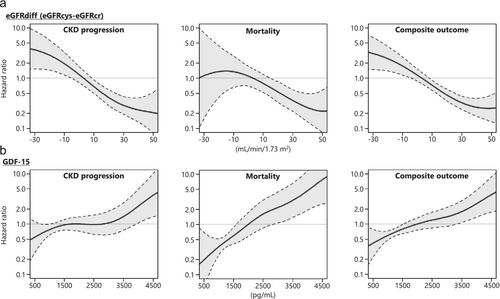
The median age was 65 years (interquartile range: 58–73), and 53.9% of participants were male. Over median follow-up periods of 5.3 years for CKD progression and 5.4 years for mortality, 75 participants (11.8%) experienced CKD progression and 44 (6.9%) died. GDF-15 levels inversely correlated with eGFRdiff (r = −0.35, p < 0.001). Higher eGFRdiff values were associated with lower odds of being in a higher GDF-15 tertile (odds ratio 0.86; 95% confidence interval [CI]: 0.76–0.97; p = 0.01). Both lower eGFRdiff and higher GDF-15 levels were independently associated with adverse outcomes: CKD progression (GDF-15, hazard ratio [HR] 1.36, 95% CI: 1.02–1.81, p < 0.05; eGFRdiff, HR 0.67, 95% CI: 0.58–0.78, p < 0.0001) and mortality (GDF-15, HR 2.35, 95% CI: 1.63–3.41, p < 0.0001; eGFRdiff: 0.80, 95% CI: 0.65–0.99, p < 0.05).
Conclusions
Both eGFRdiff and GDF-15 were independently associated with adverse outcomes in individuals with diabetes mellitus. GDF-15 showed a stronger association with mortality, whereas eGFRdiff was more strongly linked to CKD progression. These findings underscore the potential utility of these markers in risk stratification for diabetes-related complications and may guide individualized interventions in clinical practice.
期刊介绍:
The Journal of Cachexia, Sarcopenia and Muscle is a peer-reviewed international journal dedicated to publishing materials related to cachexia and sarcopenia, as well as body composition and its physiological and pathophysiological changes across the lifespan and in response to various illnesses from all fields of life sciences. The journal aims to provide a reliable resource for professionals interested in related research or involved in the clinical care of affected patients, such as those suffering from AIDS, cancer, chronic heart failure, chronic lung disease, liver cirrhosis, chronic kidney failure, rheumatoid arthritis, or sepsis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


