{"title":"妊娠在May-Hegglin异常:诊断挑战和管理考虑。","authors":"Metban Mastanzade, Alper Koç","doi":"10.1155/crh/4997232","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> May-Hegglin anomaly (MHA) is a rare autosomal dominant genetic disorder caused by mutations in the MYH9 gene, leading to the presence of Döhle-like inclusions in neutrophils, macrothrombocytes, and thrombocytopenia. This report presents a unique case of a 33-year-old pregnant woman diagnosed with MHA and discusses the diagnostic challenges and management strategies. <b>Case Presentation:</b> A 33-year-old pregnant woman, 17 weeks into her pregnancy, presented with a history of persistent thrombocytopenia. She had previously been diagnosed with immune thrombocytopenia (ITP) and treated with steroids, intravenous immunoglobulin (IVIG), and thrombopoietin receptor agonists (TPO-RA). Her platelet counts had been between 35,000 and 50,000/μL. Upon referral to the hematology clinic, her platelet count was critically low at 15,000/μL, but the mean platelet volume (MPV) remained within normal limits. Despite her low platelet count, her coagulation profile was normal, and physical examination showed no pathological findings. <b>Diagnostic Assessment:</b> The patient's blood smear revealed giant platelets and Döhle-like inclusions in the granulocytes. Genetic testing confirmed a heterozygous mutation in the MYH9 gene, leading to the diagnosis of MHA. <b>Therapeutic Intervention:</b> Due to the risks associated with thrombocytopenia in pregnancy, her prenatal care included routine platelet monitoring and a normal bleeding time assessment. The patient underwent a cesarean delivery under general anesthesia, which resulted in the birth of a healthy baby boy. <b>Conclusion:</b> The case highlights the importance of accurate diagnosis and careful monitoring in managing pregnancy in patients with MHA. A multidisciplinary approach involving obstetricians and hematologists is crucial for optimizing maternal and neonatal outcomes.</p>","PeriodicalId":46307,"journal":{"name":"Case Reports in Hematology","volume":"2025 ","pages":"4997232"},"PeriodicalIF":0.7000,"publicationDate":"2025-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12271717/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pregnancy in May-Hegglin Anomaly: Diagnostic Challenges and Management Considerations.\",\"authors\":\"Metban Mastanzade, Alper Koç\",\"doi\":\"10.1155/crh/4997232\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction:</b> May-Hegglin anomaly (MHA) is a rare autosomal dominant genetic disorder caused by mutations in the MYH9 gene, leading to the presence of Döhle-like inclusions in neutrophils, macrothrombocytes, and thrombocytopenia. This report presents a unique case of a 33-year-old pregnant woman diagnosed with MHA and discusses the diagnostic challenges and management strategies. <b>Case Presentation:</b> A 33-year-old pregnant woman, 17 weeks into her pregnancy, presented with a history of persistent thrombocytopenia. She had previously been diagnosed with immune thrombocytopenia (ITP) and treated with steroids, intravenous immunoglobulin (IVIG), and thrombopoietin receptor agonists (TPO-RA). Her platelet counts had been between 35,000 and 50,000/μL. Upon referral to the hematology clinic, her platelet count was critically low at 15,000/μL, but the mean platelet volume (MPV) remained within normal limits. Despite her low platelet count, her coagulation profile was normal, and physical examination showed no pathological findings. <b>Diagnostic Assessment:</b> The patient's blood smear revealed giant platelets and Döhle-like inclusions in the granulocytes. Genetic testing confirmed a heterozygous mutation in the MYH9 gene, leading to the diagnosis of MHA. <b>Therapeutic Intervention:</b> Due to the risks associated with thrombocytopenia in pregnancy, her prenatal care included routine platelet monitoring and a normal bleeding time assessment. The patient underwent a cesarean delivery under general anesthesia, which resulted in the birth of a healthy baby boy. <b>Conclusion:</b> The case highlights the importance of accurate diagnosis and careful monitoring in managing pregnancy in patients with MHA. A multidisciplinary approach involving obstetricians and hematologists is crucial for optimizing maternal and neonatal outcomes.</p>\",\"PeriodicalId\":46307,\"journal\":{\"name\":\"Case Reports in Hematology\",\"volume\":\"2025 \",\"pages\":\"4997232\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-07-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12271717/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/crh/4997232\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crh/4997232","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Pregnancy in May-Hegglin Anomaly: Diagnostic Challenges and Management Considerations.
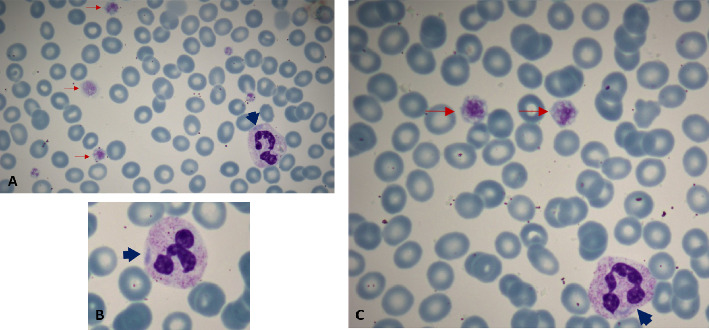
Introduction: May-Hegglin anomaly (MHA) is a rare autosomal dominant genetic disorder caused by mutations in the MYH9 gene, leading to the presence of Döhle-like inclusions in neutrophils, macrothrombocytes, and thrombocytopenia. This report presents a unique case of a 33-year-old pregnant woman diagnosed with MHA and discusses the diagnostic challenges and management strategies. Case Presentation: A 33-year-old pregnant woman, 17 weeks into her pregnancy, presented with a history of persistent thrombocytopenia. She had previously been diagnosed with immune thrombocytopenia (ITP) and treated with steroids, intravenous immunoglobulin (IVIG), and thrombopoietin receptor agonists (TPO-RA). Her platelet counts had been between 35,000 and 50,000/μL. Upon referral to the hematology clinic, her platelet count was critically low at 15,000/μL, but the mean platelet volume (MPV) remained within normal limits. Despite her low platelet count, her coagulation profile was normal, and physical examination showed no pathological findings. Diagnostic Assessment: The patient's blood smear revealed giant platelets and Döhle-like inclusions in the granulocytes. Genetic testing confirmed a heterozygous mutation in the MYH9 gene, leading to the diagnosis of MHA. Therapeutic Intervention: Due to the risks associated with thrombocytopenia in pregnancy, her prenatal care included routine platelet monitoring and a normal bleeding time assessment. The patient underwent a cesarean delivery under general anesthesia, which resulted in the birth of a healthy baby boy. Conclusion: The case highlights the importance of accurate diagnosis and careful monitoring in managing pregnancy in patients with MHA. A multidisciplinary approach involving obstetricians and hematologists is crucial for optimizing maternal and neonatal outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


