{"title":"左西孟旦治疗晚期心力衰竭患者基线特征的生存差异。","authors":"Angel-Alberto Garcia-Peña, Alejandro Mariño, Oscar-Mauricio Muñoz-Velandia, Daniela Saa-González","doi":"10.1177/20503121251357357","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>To assess whether baseline characteristics (age, New York Heart Association functional class, left ventricular ejection fraction, glomerular filtration rate, systolic blood pressure, and N-terminal pro-brain natriuretic peptide) predicted different survival functions in patients with advanced heart failure, treated with intermittent inotropics.</p><p><strong>Methods: </strong>Survival analysis based on a retrospective cohort of patients with advanced heart failure, treated with intermittent infusion of levosimendan and managed at heart failure clinic of the Hospital Universitario San Ignacio, in Bogotá (Colombia). We evaluated which baseline characteristics were associated with worse survival outcomes, using Kaplan-Meier curves and log rank test.</p><p><strong>Results: </strong>Forty-two patients with advanced heart failure were included (mean age: 69.5 ± 13.2 years, 97.6% New York Heart Association III-IV, 54.7% of the population had quadruple therapy). A total of 39.5% died during 1-year follow-up. Survival functions were worse in patients with N-terminal pro-brain natriuretic peptide levels >6000 pg/mL (HR: 2.72; 95% CI: 1.01-8.01, <i>p</i> = 0.0493). In contrast, no significant difference in mortality was found for those with basal GFR <60 versus ⩾60 ml/min (<i>p</i> = 0.1030), left ventricular ejection fraction ⩽20% versus >20% (<i>p</i> = 0.1040), systolic blood pressure <90 mmHg versus ⩾90 mmHg (<i>p</i> = 0.2463), according to functional class (<i>p</i> = 0.840) or age > 65 years (<i>p</i> = 0.169). A significant increase of left ventricular ejection fraction measurements was observed in 26 surviving patients at 12 months of follow-up (20% vs 34%, <i>p</i> < 0.0001).</p><p><strong>Conclusion: </strong>Our preliminary data suggest that the only characteristic that could predict worse survival in patients with advanced heart failure treated with levosimendan is N-terminal pro-brain natriuretic peptide levels greater than 6000 pg/ml. Future research is needed to confirm our findings.</p>","PeriodicalId":21398,"journal":{"name":"SAGE Open Medicine","volume":"13 ","pages":"20503121251357357"},"PeriodicalIF":2.1000,"publicationDate":"2025-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12276472/pdf/","citationCount":"0","resultStr":"{\"title\":\"Survival differences according to baseline characteristics of patient with advanced heart failure treated with levosimendan.\",\"authors\":\"Angel-Alberto Garcia-Peña, Alejandro Mariño, Oscar-Mauricio Muñoz-Velandia, Daniela Saa-González\",\"doi\":\"10.1177/20503121251357357\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>To assess whether baseline characteristics (age, New York Heart Association functional class, left ventricular ejection fraction, glomerular filtration rate, systolic blood pressure, and N-terminal pro-brain natriuretic peptide) predicted different survival functions in patients with advanced heart failure, treated with intermittent inotropics.</p><p><strong>Methods: </strong>Survival analysis based on a retrospective cohort of patients with advanced heart failure, treated with intermittent infusion of levosimendan and managed at heart failure clinic of the Hospital Universitario San Ignacio, in Bogotá (Colombia). We evaluated which baseline characteristics were associated with worse survival outcomes, using Kaplan-Meier curves and log rank test.</p><p><strong>Results: </strong>Forty-two patients with advanced heart failure were included (mean age: 69.5 ± 13.2 years, 97.6% New York Heart Association III-IV, 54.7% of the population had quadruple therapy). A total of 39.5% died during 1-year follow-up. Survival functions were worse in patients with N-terminal pro-brain natriuretic peptide levels >6000 pg/mL (HR: 2.72; 95% CI: 1.01-8.01, <i>p</i> = 0.0493). In contrast, no significant difference in mortality was found for those with basal GFR <60 versus ⩾60 ml/min (<i>p</i> = 0.1030), left ventricular ejection fraction ⩽20% versus >20% (<i>p</i> = 0.1040), systolic blood pressure <90 mmHg versus ⩾90 mmHg (<i>p</i> = 0.2463), according to functional class (<i>p</i> = 0.840) or age > 65 years (<i>p</i> = 0.169). A significant increase of left ventricular ejection fraction measurements was observed in 26 surviving patients at 12 months of follow-up (20% vs 34%, <i>p</i> < 0.0001).</p><p><strong>Conclusion: </strong>Our preliminary data suggest that the only characteristic that could predict worse survival in patients with advanced heart failure treated with levosimendan is N-terminal pro-brain natriuretic peptide levels greater than 6000 pg/ml. Future research is needed to confirm our findings.</p>\",\"PeriodicalId\":21398,\"journal\":{\"name\":\"SAGE Open Medicine\",\"volume\":\"13 \",\"pages\":\"20503121251357357\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-07-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12276472/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"SAGE Open Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20503121251357357\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAGE Open Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20503121251357357","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Survival differences according to baseline characteristics of patient with advanced heart failure treated with levosimendan.
Aims: To assess whether baseline characteristics (age, New York Heart Association functional class, left ventricular ejection fraction, glomerular filtration rate, systolic blood pressure, and N-terminal pro-brain natriuretic peptide) predicted different survival functions in patients with advanced heart failure, treated with intermittent inotropics.
Methods: Survival analysis based on a retrospective cohort of patients with advanced heart failure, treated with intermittent infusion of levosimendan and managed at heart failure clinic of the Hospital Universitario San Ignacio, in Bogotá (Colombia). We evaluated which baseline characteristics were associated with worse survival outcomes, using Kaplan-Meier curves and log rank test.
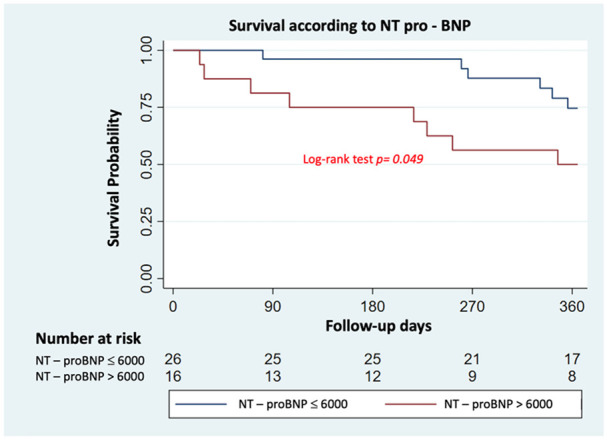
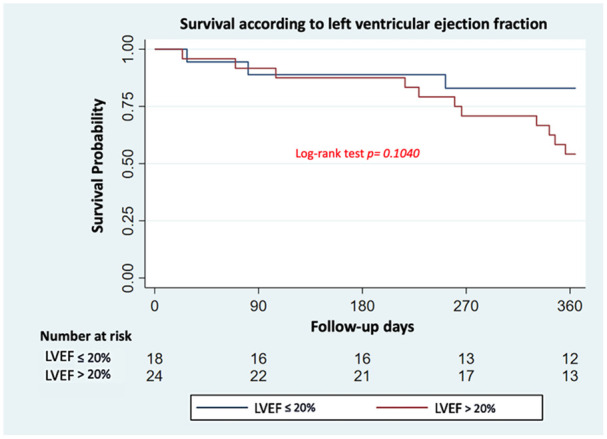
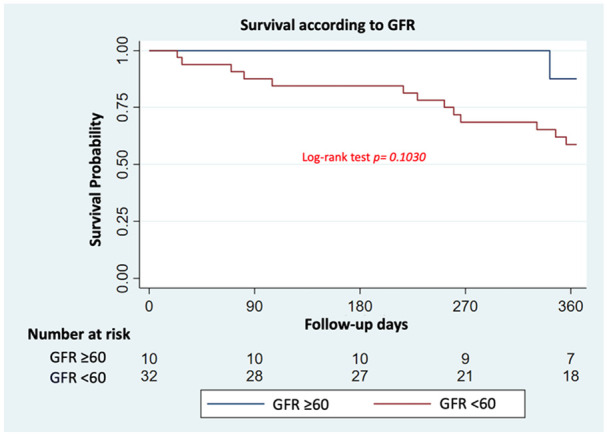
Results: Forty-two patients with advanced heart failure were included (mean age: 69.5 ± 13.2 years, 97.6% New York Heart Association III-IV, 54.7% of the population had quadruple therapy). A total of 39.5% died during 1-year follow-up. Survival functions were worse in patients with N-terminal pro-brain natriuretic peptide levels >6000 pg/mL (HR: 2.72; 95% CI: 1.01-8.01, p = 0.0493). In contrast, no significant difference in mortality was found for those with basal GFR <60 versus ⩾60 ml/min (p = 0.1030), left ventricular ejection fraction ⩽20% versus >20% (p = 0.1040), systolic blood pressure <90 mmHg versus ⩾90 mmHg (p = 0.2463), according to functional class (p = 0.840) or age > 65 years (p = 0.169). A significant increase of left ventricular ejection fraction measurements was observed in 26 surviving patients at 12 months of follow-up (20% vs 34%, p < 0.0001).
Conclusion: Our preliminary data suggest that the only characteristic that could predict worse survival in patients with advanced heart failure treated with levosimendan is N-terminal pro-brain natriuretic peptide levels greater than 6000 pg/ml. Future research is needed to confirm our findings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


