{"title":"缩小塞内加尔孕期疟疾护理方面的城乡差距:来自家庭和卫生设施调查的证据。","authors":"Yongsheng Jiang, Di Liang, Jinkou Zhao, Shailendra Prasad, Medoune Ndiop, Serigne Amdy Thiam, Ibrahima Diallo, Doudou Sene, Rose Mpembeni, Jiayan Huang","doi":"10.1186/s40249-025-01341-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite the World Health Organization's recommendations, the uptake of Intermittent Preventive Treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP) in Senegal remains suboptimal, with disparities observed between urban and rural areas. More remains to be known about how malaria service readiness would affect the utilization of IPTp-SP.</p><p><strong>Methods: </strong>Data were obtained from seven annual rounds of Demographic and Health Surveys (DHS) and Service Provision Assessments (SPA) in Senegal from 2012 to 2019. Using sample domain linkage to link the databases at the regional level. A malaria service readiness index was calculated to quantify the malaria service delivery capacity within the service environment where women reside. The Heckman selection model was utilized to analyze the relationship between malaria service readiness and IPTp-SP utilization.</p><p><strong>Results: </strong>From 2012 to 2019, the average number of IPTp-SP doses received in Senegal was 1.66 (95% CI: 1.65-1.68), higher in urban areas [1.73 (95% CI: 1.71-1.75)] than rural areas [1.63 (95% CI: 1.62-1.65)]. Each one-point increase in malaria service readiness led to a rise of 0.251 doses in IPTp-SP. The significant interaction (Coef. = - 0.523, P < 0.001) indicated that women in rural areas received fewer doses of IPTp-SP (0.089) than in urban areas (0.612) for every unit increase in malaria service readiness.</p><p><strong>Conclusions: </strong>Linking household and health facility surveys revealed significant room for improvement in malaria service readiness and IPTp-SP utilization in rural areas in Senegal. For better IPTp-SP coverage, differential strategies are required for urban and rural settings. Urban areas need to enhance malaria service readiness, while rural areas should focus on improving service readiness alongside infrastructure and community engagement to bridge the urban-rural disparities.</p>","PeriodicalId":48820,"journal":{"name":"Infectious Diseases of Poverty","volume":"14 1","pages":"71"},"PeriodicalIF":5.5000,"publicationDate":"2025-07-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12276681/pdf/","citationCount":"0","resultStr":"{\"title\":\"Bridging urban-rural disparities in malaria care during pregnancy in Senegal: evidence from household and health facility surveys.\",\"authors\":\"Yongsheng Jiang, Di Liang, Jinkou Zhao, Shailendra Prasad, Medoune Ndiop, Serigne Amdy Thiam, Ibrahima Diallo, Doudou Sene, Rose Mpembeni, Jiayan Huang\",\"doi\":\"10.1186/s40249-025-01341-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Despite the World Health Organization's recommendations, the uptake of Intermittent Preventive Treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP) in Senegal remains suboptimal, with disparities observed between urban and rural areas. More remains to be known about how malaria service readiness would affect the utilization of IPTp-SP.</p><p><strong>Methods: </strong>Data were obtained from seven annual rounds of Demographic and Health Surveys (DHS) and Service Provision Assessments (SPA) in Senegal from 2012 to 2019. Using sample domain linkage to link the databases at the regional level. A malaria service readiness index was calculated to quantify the malaria service delivery capacity within the service environment where women reside. The Heckman selection model was utilized to analyze the relationship between malaria service readiness and IPTp-SP utilization.</p><p><strong>Results: </strong>From 2012 to 2019, the average number of IPTp-SP doses received in Senegal was 1.66 (95% CI: 1.65-1.68), higher in urban areas [1.73 (95% CI: 1.71-1.75)] than rural areas [1.63 (95% CI: 1.62-1.65)]. Each one-point increase in malaria service readiness led to a rise of 0.251 doses in IPTp-SP. The significant interaction (Coef. = - 0.523, P < 0.001) indicated that women in rural areas received fewer doses of IPTp-SP (0.089) than in urban areas (0.612) for every unit increase in malaria service readiness.</p><p><strong>Conclusions: </strong>Linking household and health facility surveys revealed significant room for improvement in malaria service readiness and IPTp-SP utilization in rural areas in Senegal. For better IPTp-SP coverage, differential strategies are required for urban and rural settings. Urban areas need to enhance malaria service readiness, while rural areas should focus on improving service readiness alongside infrastructure and community engagement to bridge the urban-rural disparities.</p>\",\"PeriodicalId\":48820,\"journal\":{\"name\":\"Infectious Diseases of Poverty\",\"volume\":\"14 1\",\"pages\":\"71\"},\"PeriodicalIF\":5.5000,\"publicationDate\":\"2025-07-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12276681/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Infectious Diseases of Poverty\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40249-025-01341-5\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Diseases of Poverty","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40249-025-01341-5","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Bridging urban-rural disparities in malaria care during pregnancy in Senegal: evidence from household and health facility surveys.
Background: Despite the World Health Organization's recommendations, the uptake of Intermittent Preventive Treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP) in Senegal remains suboptimal, with disparities observed between urban and rural areas. More remains to be known about how malaria service readiness would affect the utilization of IPTp-SP.
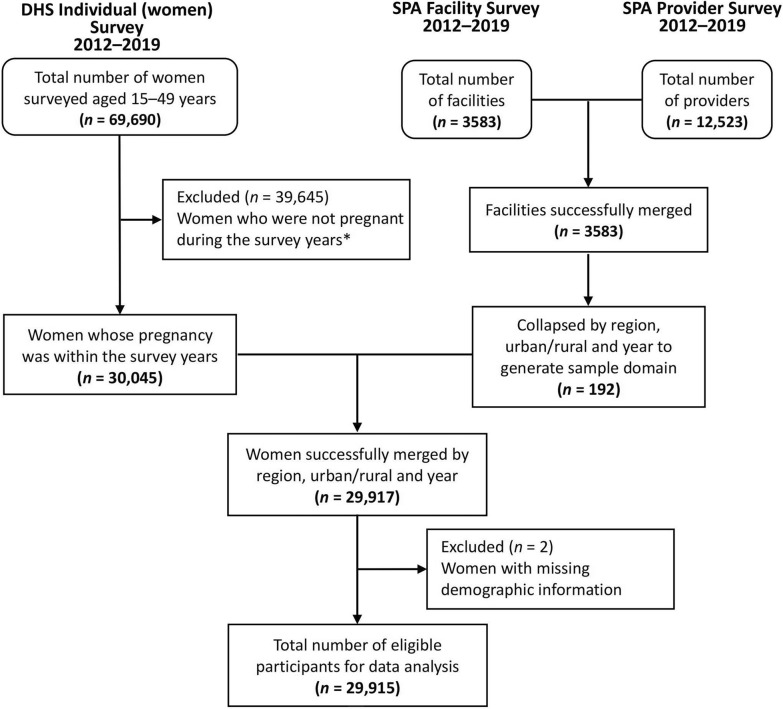
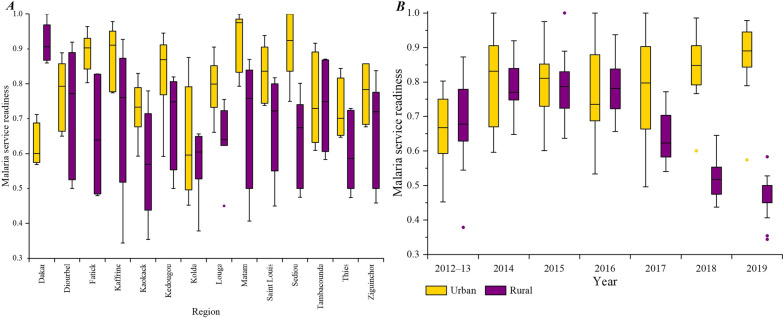
Methods: Data were obtained from seven annual rounds of Demographic and Health Surveys (DHS) and Service Provision Assessments (SPA) in Senegal from 2012 to 2019. Using sample domain linkage to link the databases at the regional level. A malaria service readiness index was calculated to quantify the malaria service delivery capacity within the service environment where women reside. The Heckman selection model was utilized to analyze the relationship between malaria service readiness and IPTp-SP utilization.
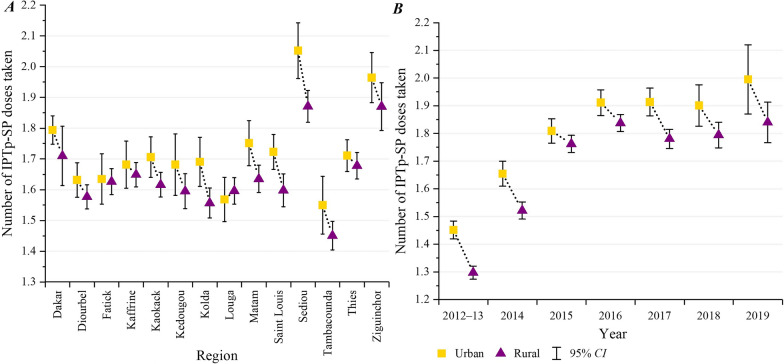
Results: From 2012 to 2019, the average number of IPTp-SP doses received in Senegal was 1.66 (95% CI: 1.65-1.68), higher in urban areas [1.73 (95% CI: 1.71-1.75)] than rural areas [1.63 (95% CI: 1.62-1.65)]. Each one-point increase in malaria service readiness led to a rise of 0.251 doses in IPTp-SP. The significant interaction (Coef. = - 0.523, P < 0.001) indicated that women in rural areas received fewer doses of IPTp-SP (0.089) than in urban areas (0.612) for every unit increase in malaria service readiness.
Conclusions: Linking household and health facility surveys revealed significant room for improvement in malaria service readiness and IPTp-SP utilization in rural areas in Senegal. For better IPTp-SP coverage, differential strategies are required for urban and rural settings. Urban areas need to enhance malaria service readiness, while rural areas should focus on improving service readiness alongside infrastructure and community engagement to bridge the urban-rural disparities.
期刊介绍:
Infectious Diseases of Poverty is an open access, peer-reviewed journal that focuses on addressing essential public health questions related to infectious diseases of poverty. The journal covers a wide range of topics including the biology of pathogens and vectors, diagnosis and detection, treatment and case management, epidemiology and modeling, zoonotic hosts and animal reservoirs, control strategies and implementation, new technologies and application. It also considers the transdisciplinary or multisectoral effects on health systems, ecohealth, environmental management, and innovative technology. The journal aims to identify and assess research and information gaps that hinder progress towards new interventions for public health problems in the developing world. Additionally, it provides a platform for discussing these issues to advance research and evidence building for improved public health interventions in poor settings.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


