Fabian Maximilian Meinert, Jenny Dimakos, Thomas Günther Riemer, Antonios Douros
{"title":"直接口服抗凝剂和抗心律失常药物同时使用的有效性和安全性:观察性研究的系统回顾。","authors":"Fabian Maximilian Meinert, Jenny Dimakos, Thomas Günther Riemer, Antonios Douros","doi":"10.1007/s00228-025-03883-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Concomitant use of antiarrhythmic drugs (AAs) may affect the effectiveness and safety of direct oral anticoagulants (DOACs) through pharmacokinetic interactions and other factors. Our systematic review aimed to provide an in-depth methodological assessment and synthesis of the available real-world evidence in the area.</p><p><strong>Methods: </strong>We systematically searched MEDLINE/PubMed and EMBASE from January 2011 to October 2024 for observational studies assessing the effectiveness (risk of stroke) and safety (risk of major bleeding) associated with concomitant use of DOACs and AAs. We assessed the risk of bias using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool.</p><p><strong>Results: </strong>We identified 17 relevant studies including overall 2,613,693 patients. For stroke, all six studies showed no increased risk associated with concomitant use of DOACs and AAs. For major bleeding, seven studies showed an increased risk associated with concomitant use of DOACs and AAs (up to 187%), four studies showed heterogeneous results depending on the specific AA, and six studies showed no increased risk. When considering only higher-quality studies (n = 6), there was no association with the risk of stroke (n = 3). There were associations with an increased risk of major bleeding for concomitant use of DOACs and diltiazem (n = 2) or verapamil (n = 1), while findings for concomitant use of DOACs and amiodarone were inconsistent (n = 3).</p><p><strong>Conclusions: </strong>Based on the synthesis of higher-quality real-world evidence, concomitant use of AAs does not seem to impact the effectiveness of DOACs. Findings on safety possibly depend on the specific AA, with diltiazem showing the highest risk.</p>","PeriodicalId":11857,"journal":{"name":"European Journal of Clinical Pharmacology","volume":" ","pages":"1409-1419"},"PeriodicalIF":2.7000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12443910/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effectiveness and safety of concomitant use of direct oral anticoagulants and antiarrhythmic drugs: a systematic review of observational studies.\",\"authors\":\"Fabian Maximilian Meinert, Jenny Dimakos, Thomas Günther Riemer, Antonios Douros\",\"doi\":\"10.1007/s00228-025-03883-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Concomitant use of antiarrhythmic drugs (AAs) may affect the effectiveness and safety of direct oral anticoagulants (DOACs) through pharmacokinetic interactions and other factors. Our systematic review aimed to provide an in-depth methodological assessment and synthesis of the available real-world evidence in the area.</p><p><strong>Methods: </strong>We systematically searched MEDLINE/PubMed and EMBASE from January 2011 to October 2024 for observational studies assessing the effectiveness (risk of stroke) and safety (risk of major bleeding) associated with concomitant use of DOACs and AAs. We assessed the risk of bias using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool.</p><p><strong>Results: </strong>We identified 17 relevant studies including overall 2,613,693 patients. For stroke, all six studies showed no increased risk associated with concomitant use of DOACs and AAs. For major bleeding, seven studies showed an increased risk associated with concomitant use of DOACs and AAs (up to 187%), four studies showed heterogeneous results depending on the specific AA, and six studies showed no increased risk. When considering only higher-quality studies (n = 6), there was no association with the risk of stroke (n = 3). There were associations with an increased risk of major bleeding for concomitant use of DOACs and diltiazem (n = 2) or verapamil (n = 1), while findings for concomitant use of DOACs and amiodarone were inconsistent (n = 3).</p><p><strong>Conclusions: </strong>Based on the synthesis of higher-quality real-world evidence, concomitant use of AAs does not seem to impact the effectiveness of DOACs. Findings on safety possibly depend on the specific AA, with diltiazem showing the highest risk.</p>\",\"PeriodicalId\":11857,\"journal\":{\"name\":\"European Journal of Clinical Pharmacology\",\"volume\":\" \",\"pages\":\"1409-1419\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12443910/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Clinical Pharmacology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00228-025-03883-x\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Clinical Pharmacology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00228-025-03883-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Effectiveness and safety of concomitant use of direct oral anticoagulants and antiarrhythmic drugs: a systematic review of observational studies.
Introduction: Concomitant use of antiarrhythmic drugs (AAs) may affect the effectiveness and safety of direct oral anticoagulants (DOACs) through pharmacokinetic interactions and other factors. Our systematic review aimed to provide an in-depth methodological assessment and synthesis of the available real-world evidence in the area.
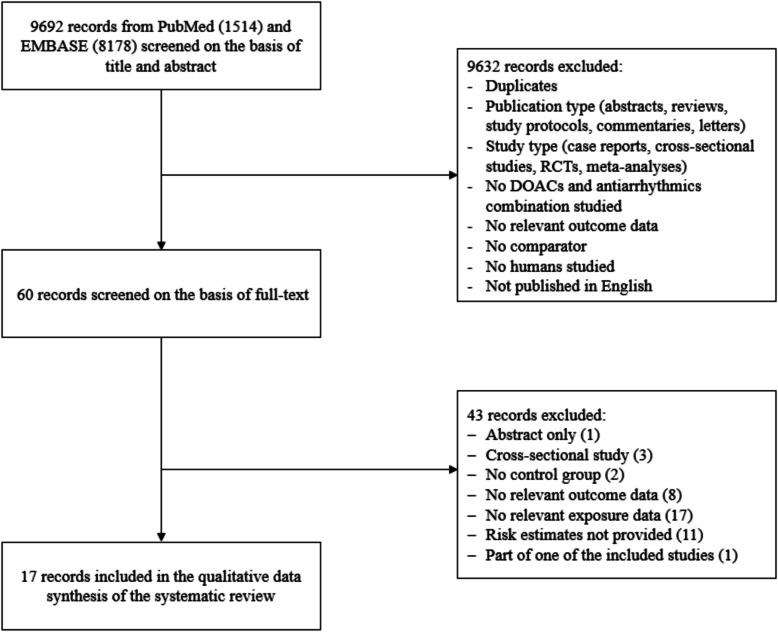
Methods: We systematically searched MEDLINE/PubMed and EMBASE from January 2011 to October 2024 for observational studies assessing the effectiveness (risk of stroke) and safety (risk of major bleeding) associated with concomitant use of DOACs and AAs. We assessed the risk of bias using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool.
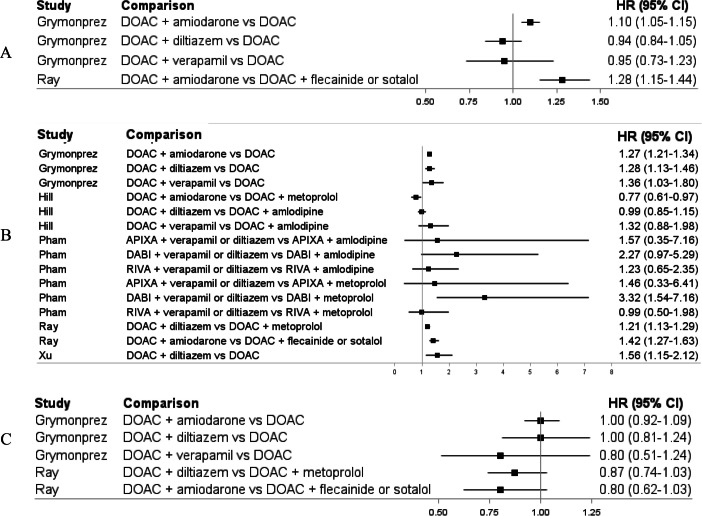
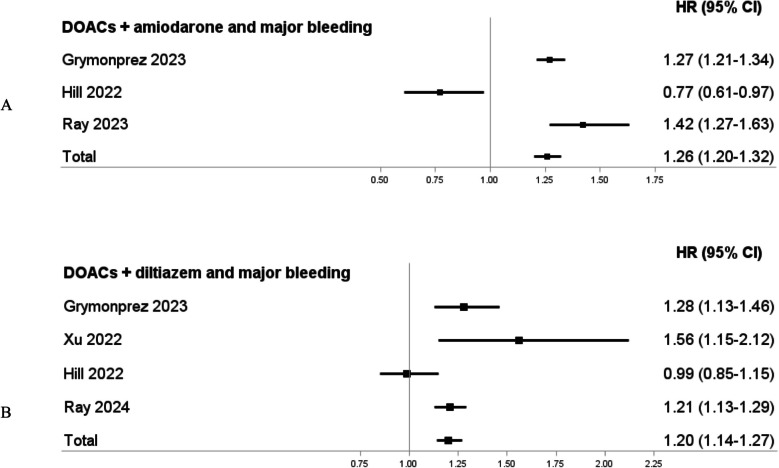
Results: We identified 17 relevant studies including overall 2,613,693 patients. For stroke, all six studies showed no increased risk associated with concomitant use of DOACs and AAs. For major bleeding, seven studies showed an increased risk associated with concomitant use of DOACs and AAs (up to 187%), four studies showed heterogeneous results depending on the specific AA, and six studies showed no increased risk. When considering only higher-quality studies (n = 6), there was no association with the risk of stroke (n = 3). There were associations with an increased risk of major bleeding for concomitant use of DOACs and diltiazem (n = 2) or verapamil (n = 1), while findings for concomitant use of DOACs and amiodarone were inconsistent (n = 3).
Conclusions: Based on the synthesis of higher-quality real-world evidence, concomitant use of AAs does not seem to impact the effectiveness of DOACs. Findings on safety possibly depend on the specific AA, with diltiazem showing the highest risk.
期刊介绍:
The European Journal of Clinical Pharmacology publishes original papers on all aspects of clinical pharmacology and drug therapy in humans. Manuscripts are welcomed on the following topics: therapeutic trials, pharmacokinetics/pharmacodynamics, pharmacogenetics, drug metabolism, adverse drug reactions, drug interactions, all aspects of drug development, development relating to teaching in clinical pharmacology, pharmacoepidemiology, and matters relating to the rational prescribing and safe use of drugs. Methodological contributions relevant to these topics are also welcomed.
Data from animal experiments are accepted only in the context of original data in man reported in the same paper. EJCP will only consider manuscripts describing the frequency of allelic variants in different populations if this information is linked to functional data or new interesting variants. Highly relevant differences in frequency with a major impact in drug therapy for the respective population may be submitted as a letter to the editor.
Straightforward phase I pharmacokinetic or pharmacodynamic studies as parts of new drug development will only be considered for publication if the paper involves
-a compound that is interesting and new in some basic or fundamental way, or
-methods that are original in some basic sense, or
-a highly unexpected outcome, or
-conclusions that are scientifically novel in some basic or fundamental sense.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


