Floor Nh Wilting, Lotte Sondag, Floris Hbm Schreuder, Ruben Dammers, Catharina Jm Klijn, Hieronymus D Boogaarts
{"title":"自发性幕上脑出血的外科治疗。","authors":"Floor Nh Wilting, Lotte Sondag, Floris Hbm Schreuder, Ruben Dammers, Catharina Jm Klijn, Hieronymus D Boogaarts","doi":"10.1002/14651858.CD015387.pub2","DOIUrl":null,"url":null,"abstract":"<p><strong>Rationale: </strong>It is unknown whether surgery improves outcomes in people with spontaneous supratentorial intracerebral haemorrhage (ICH), and whether the effects of surgery differ according to the applied surgical technique. This review updated the methodology of a previous Cochrane review from 2008.</p><p><strong>Objectives: </strong>To assess the benefits and harms of surgery plus standard medical management, compared to standard medical management alone, in people with spontaneous supratentorial ICH, and to assess whether the effect of surgery differs according to the surgical technique used.</p><p><strong>Search methods: </strong>We searched Cochrane Stroke Group Trials Register, CENTRAL, MEDLINE, and five other databases to 11 March 2025. We handsearched reference lists of included studies and relevant systematic reviews, forward-tracked relevant references, and contacted trialists for additional information on unpublished or ongoing studies.</p><p><strong>Eligibility criteria: </strong>We included randomised controlled trials (RCTs) of surgery (craniotomy with haematoma evacuation, minimally invasive surgery (MIS), or decompressive craniectomy) plus standard medical management in adults with a spontaneous supratentorial ICH, compared with standard medical management alone. We excluded studies of people with secondary causes of ICH (such as trauma, a macrovascular cause, or an intracranial tumour).</p><p><strong>Outcomes: </strong>Critical outcomes were: good functional outcome at end of scheduled follow-up, and all-cause mortality at end of scheduled follow-up. Important outcomes were: 30-day case fatality and health-related quality of life (HRQoL) at end of scheduled follow-up.</p><p><strong>Risk of bias: </strong>We used the Cochrane RoB 1 tool.</p><p><strong>Synthesis methods: </strong>We conducted meta-analyses using random-effects models to calculate risk ratios (RR) with 95% confidence intervals (CI) for dichotomous data, and mean differences (MD) with 95% CI for continuous data. We summarised the certainty of the evidence using GRADE.</p><p><strong>Included studies: </strong>We included 24 RCTs (4597 participants). The studies were conducted in Europe, North and South America, Asia, Africa, and Australia, and were published between 1989 and 2024. Twenty-three studies examined surgery aimed at clot removal plus standard medical management versus standard medical management, of which six were included in the separate comparison of craniotomy with haematoma evacuation plus standard medical management versus standard medical management, and 14 in the comparison of MIS plus standard medical management versus standard medical management. One study examined decompressive craniectomy without haematoma evacuation plus standard medical management versus standard medical management.</p><p><strong>Synthesis of results: </strong>Surgery aimed at clot removal plus standard medical management versus standard medical management alone Low-certainty evidence suggests that surgery aimed at clot removal may increase the chance of good functional outcome (RR 1.30, 95% CI 1.15 to 1.47; 18 studies, 4043 participants), and may reduce all-cause mortality (RR 0.79, 95% CI 0.71 to 0.88; 22 studies, 4278 participants) and 30-day case fatality (RR 0.74, 95% CI 0.60 to 0.90; 11 studies, 3179 participants). Surgery aimed at clot removal may have little to no effect on HRQoL, but the evidence is very uncertain (MD 0.03, 95% CI -0.05 to 0.11; 2 studies, 472 participants). Craniotomy with haematoma evacuation plus standard medical management versus standard medical management alone Craniotomy with haematoma evacuation may increase the chance of good functional outcome, but the evidence is very uncertain (RR 1.41, 95% CI 0.77 to 2.55; 6 studies, 853 participants). Craniotomy with haematoma evacuation likely reduces all-cause mortality (RR 0.80, 95% CI 0.67 to 0.96; 5 studies, 845 participants; moderate-certainty evidence), and may reduce 30-day case fatality (RR 0.68, 95% CI 0.46 to 1.00; 3 studies, 676 participants; low-certainty evidence), but the pooled CIs of 30-day case fatality included the possibility of no effect. Craniotomy with haematoma evacuation may result in little to no difference in HRQoL (MD 0.04, 95% CI -0.04 to 0.12; 1 study, 445 participants; low-certainty evidence). Minimally invasive surgery plus standard medical management versus standard medical management alone MIS may increase the chance of good functional outcome (RR 1.36, 95% CI 1.18 to 1.58; 10 studies, 2218 participants; low-certainty evidence), and probably reduces all-cause mortality (RR 0.71, 95% CI 0.60 to 0.84; 14 studies, 2401 participants; moderate-certainty evidence) and 30-day case fatality (RR 0.62, 95% CI 0.47 to 0.81; 7 studies, 1521 participants; moderate-certainty evidence). The evidence is very uncertain about HRQoL (MD -0.14, 95% CI -0.50 to 0.22; 1 study, 27 participants). Decompressive craniectomy plus standard medical management versus standard medical management alone Based on low-certainty evidence from one study, decompressive craniectomy may increase the chance of good functional outcome (RR 1.23, 95% CI 0.65 to 2.32; 182 participants), may reduce all-cause mortality (RR 0.74, 95% CI 0.45 to 1.19; 197 participants), and may result in little to no difference in HRQoL (MD 0.01, 95% CI -0.13 to 0.14), but the pooled CIs for these outcomes included the possibility of both benefit and harm. Decompressive craniectomy may also reduce 30-day case fatality, but the pooled CIs included the possibility of no effect (RR 0.43, 95% CI 0.19 to 1.00; 197 participants; low-certainty evidence).</p><p><strong>Authors' conclusions: </strong>For people with spontaneous supratentorial ICH, surgery aimed at clot removal may increase the chance of achieving good functional outcome and may reduce all-cause mortality and 30-day case fatality compared to standard medical management. When the results are divided by neurosurgical approach for haematoma evacuation, craniotomy likely reduces all-cause mortality and may reduce 30-day case fatality, while its effect on good functional outcome is very uncertain. MIS may increase the chance of good functional outcome, and probably reduces all-cause mortality and 30-day case fatality. Although the effect estimates for all outcomes regarding decompressive craniectomy may suggest a beneficial effect, the pooled estimates were very imprecise and included the possibility of a harmful (good functional outcome and all-cause mortality) or no effect (30-day case fatality). Evidence on HRQoL was low or very low certainty, overall, and for each surgical technique. The certainty of the evidence was limited due to methodological shortcomings and the high risk of bias of most included studies, as well as imprecise pooled estimates and substantial heterogeneity in some analyses. More high-quality and adequately powered studies are needed to be more certain and to guide clinical practice.</p><p><strong>Funding: </strong>This Cochrane review had no dedicated funding.</p><p><strong>Registration: </strong>Protocol (2022) available via doi.org/10.1002/14651858.CD015387.</p>","PeriodicalId":10473,"journal":{"name":"Cochrane Database of Systematic Reviews","volume":"7 ","pages":"CD015387"},"PeriodicalIF":8.8000,"publicationDate":"2025-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12269361/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgery for spontaneous supratentorial intracerebral haemorrhage.\",\"authors\":\"Floor Nh Wilting, Lotte Sondag, Floris Hbm Schreuder, Ruben Dammers, Catharina Jm Klijn, Hieronymus D Boogaarts\",\"doi\":\"10.1002/14651858.CD015387.pub2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Rationale: </strong>It is unknown whether surgery improves outcomes in people with spontaneous supratentorial intracerebral haemorrhage (ICH), and whether the effects of surgery differ according to the applied surgical technique. This review updated the methodology of a previous Cochrane review from 2008.</p><p><strong>Objectives: </strong>To assess the benefits and harms of surgery plus standard medical management, compared to standard medical management alone, in people with spontaneous supratentorial ICH, and to assess whether the effect of surgery differs according to the surgical technique used.</p><p><strong>Search methods: </strong>We searched Cochrane Stroke Group Trials Register, CENTRAL, MEDLINE, and five other databases to 11 March 2025. We handsearched reference lists of included studies and relevant systematic reviews, forward-tracked relevant references, and contacted trialists for additional information on unpublished or ongoing studies.</p><p><strong>Eligibility criteria: </strong>We included randomised controlled trials (RCTs) of surgery (craniotomy with haematoma evacuation, minimally invasive surgery (MIS), or decompressive craniectomy) plus standard medical management in adults with a spontaneous supratentorial ICH, compared with standard medical management alone. We excluded studies of people with secondary causes of ICH (such as trauma, a macrovascular cause, or an intracranial tumour).</p><p><strong>Outcomes: </strong>Critical outcomes were: good functional outcome at end of scheduled follow-up, and all-cause mortality at end of scheduled follow-up. Important outcomes were: 30-day case fatality and health-related quality of life (HRQoL) at end of scheduled follow-up.</p><p><strong>Risk of bias: </strong>We used the Cochrane RoB 1 tool.</p><p><strong>Synthesis methods: </strong>We conducted meta-analyses using random-effects models to calculate risk ratios (RR) with 95% confidence intervals (CI) for dichotomous data, and mean differences (MD) with 95% CI for continuous data. We summarised the certainty of the evidence using GRADE.</p><p><strong>Included studies: </strong>We included 24 RCTs (4597 participants). The studies were conducted in Europe, North and South America, Asia, Africa, and Australia, and were published between 1989 and 2024. Twenty-three studies examined surgery aimed at clot removal plus standard medical management versus standard medical management, of which six were included in the separate comparison of craniotomy with haematoma evacuation plus standard medical management versus standard medical management, and 14 in the comparison of MIS plus standard medical management versus standard medical management. One study examined decompressive craniectomy without haematoma evacuation plus standard medical management versus standard medical management.</p><p><strong>Synthesis of results: </strong>Surgery aimed at clot removal plus standard medical management versus standard medical management alone Low-certainty evidence suggests that surgery aimed at clot removal may increase the chance of good functional outcome (RR 1.30, 95% CI 1.15 to 1.47; 18 studies, 4043 participants), and may reduce all-cause mortality (RR 0.79, 95% CI 0.71 to 0.88; 22 studies, 4278 participants) and 30-day case fatality (RR 0.74, 95% CI 0.60 to 0.90; 11 studies, 3179 participants). Surgery aimed at clot removal may have little to no effect on HRQoL, but the evidence is very uncertain (MD 0.03, 95% CI -0.05 to 0.11; 2 studies, 472 participants). Craniotomy with haematoma evacuation plus standard medical management versus standard medical management alone Craniotomy with haematoma evacuation may increase the chance of good functional outcome, but the evidence is very uncertain (RR 1.41, 95% CI 0.77 to 2.55; 6 studies, 853 participants). Craniotomy with haematoma evacuation likely reduces all-cause mortality (RR 0.80, 95% CI 0.67 to 0.96; 5 studies, 845 participants; moderate-certainty evidence), and may reduce 30-day case fatality (RR 0.68, 95% CI 0.46 to 1.00; 3 studies, 676 participants; low-certainty evidence), but the pooled CIs of 30-day case fatality included the possibility of no effect. Craniotomy with haematoma evacuation may result in little to no difference in HRQoL (MD 0.04, 95% CI -0.04 to 0.12; 1 study, 445 participants; low-certainty evidence). Minimally invasive surgery plus standard medical management versus standard medical management alone MIS may increase the chance of good functional outcome (RR 1.36, 95% CI 1.18 to 1.58; 10 studies, 2218 participants; low-certainty evidence), and probably reduces all-cause mortality (RR 0.71, 95% CI 0.60 to 0.84; 14 studies, 2401 participants; moderate-certainty evidence) and 30-day case fatality (RR 0.62, 95% CI 0.47 to 0.81; 7 studies, 1521 participants; moderate-certainty evidence). The evidence is very uncertain about HRQoL (MD -0.14, 95% CI -0.50 to 0.22; 1 study, 27 participants). Decompressive craniectomy plus standard medical management versus standard medical management alone Based on low-certainty evidence from one study, decompressive craniectomy may increase the chance of good functional outcome (RR 1.23, 95% CI 0.65 to 2.32; 182 participants), may reduce all-cause mortality (RR 0.74, 95% CI 0.45 to 1.19; 197 participants), and may result in little to no difference in HRQoL (MD 0.01, 95% CI -0.13 to 0.14), but the pooled CIs for these outcomes included the possibility of both benefit and harm. Decompressive craniectomy may also reduce 30-day case fatality, but the pooled CIs included the possibility of no effect (RR 0.43, 95% CI 0.19 to 1.00; 197 participants; low-certainty evidence).</p><p><strong>Authors' conclusions: </strong>For people with spontaneous supratentorial ICH, surgery aimed at clot removal may increase the chance of achieving good functional outcome and may reduce all-cause mortality and 30-day case fatality compared to standard medical management. When the results are divided by neurosurgical approach for haematoma evacuation, craniotomy likely reduces all-cause mortality and may reduce 30-day case fatality, while its effect on good functional outcome is very uncertain. MIS may increase the chance of good functional outcome, and probably reduces all-cause mortality and 30-day case fatality. Although the effect estimates for all outcomes regarding decompressive craniectomy may suggest a beneficial effect, the pooled estimates were very imprecise and included the possibility of a harmful (good functional outcome and all-cause mortality) or no effect (30-day case fatality). Evidence on HRQoL was low or very low certainty, overall, and for each surgical technique. The certainty of the evidence was limited due to methodological shortcomings and the high risk of bias of most included studies, as well as imprecise pooled estimates and substantial heterogeneity in some analyses. More high-quality and adequately powered studies are needed to be more certain and to guide clinical practice.</p><p><strong>Funding: </strong>This Cochrane review had no dedicated funding.</p><p><strong>Registration: </strong>Protocol (2022) available via doi.org/10.1002/14651858.CD015387.</p>\",\"PeriodicalId\":10473,\"journal\":{\"name\":\"Cochrane Database of Systematic Reviews\",\"volume\":\"7 \",\"pages\":\"CD015387\"},\"PeriodicalIF\":8.8000,\"publicationDate\":\"2025-07-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12269361/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cochrane Database of Systematic Reviews\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/14651858.CD015387.pub2\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cochrane Database of Systematic Reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/14651858.CD015387.pub2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
理由:目前尚不清楚手术是否能改善自发性幕上脑出血(ICH)患者的预后,以及手术效果是否因手术技术的不同而不同。本综述更新了2008年Cochrane综述的方法。目的:评估自发性幕上脑出血患者手术加标准医疗管理与单独标准医疗管理相比的利弊,并评估手术效果是否因手术技术的不同而不同。检索方法:我们检索了Cochrane卒中组试验注册、CENTRAL、MEDLINE和其他5个数据库,截止到2025年3月11日。我们手工检索纳入研究和相关系统综述的参考文献列表,前瞻性追踪相关参考文献,并联系试验人员获取未发表或正在进行的研究的额外信息。入选标准:我们纳入了随机对照试验(RCTs),将自发性幕上脑出血成人手术(开颅血肿清除术、微创手术(MIS)或减压开颅)加标准药物治疗与单独标准药物治疗进行比较。我们排除了继发性脑出血(如创伤、大血管原因或颅内肿瘤)患者的研究。结果:关键结果为:随访结束时功能良好,随访结束时全因死亡率。重要的结局是:在预定随访结束时30天病死率和健康相关生活质量(HRQoL)。偏倚风险:我们使用Cochrane RoB 1工具。综合方法:我们使用随机效应模型进行meta分析,以95%置信区间(CI)计算二分类数据的风险比(RR),以95%置信区间(CI)计算连续数据的平均差异(MD)。我们用GRADE来总结证据的确定性。纳入研究:纳入24项随机对照试验(4597名受试者)。这些研究在欧洲、北美和南美、亚洲、非洲和澳大利亚进行,并于1989年至2024年间发表。23项研究检查了以血块清除+标准医疗管理与标准医疗管理为目的的手术,其中6项研究分别比较了开颅手术+血肿清除+标准医疗管理与标准医疗管理,14项研究比较了MIS +标准医疗管理与标准医疗管理。一项研究检查了无血肿清除的减压颅骨切除术加标准医疗管理与标准医疗管理的对比。结果综合:以血块清除为目的的手术加上标准医疗管理与单独的标准医疗管理相比,低确定性证据表明,以血块清除为目的的手术可能增加良好功能结局的机会(RR 1.30, 95% CI 1.15至1.47;18项研究,4043名受试者),并可能降低全因死亡率(RR 0.79, 95% CI 0.71 - 0.88;22项研究,4278名受试者)和30天病死率(RR 0.74, 95% CI 0.60 ~ 0.90;11项研究,3179名参与者)。旨在清除血块的手术可能对HRQoL几乎没有影响,但证据非常不确定(MD 0.03, 95% CI -0.05 ~ 0.11;2项研究,472名参与者)。开颅术+血肿清除+标准医疗处理与单独标准医疗处理相比,开颅术+血肿清除可能增加良好功能结局的机会,但证据非常不确定(RR 1.41, 95% CI 0.77 ~ 2.55;6项研究,853名参与者)。开颅手术合并血肿清除可能降低全因死亡率(RR 0.80, 95% CI 0.67 - 0.96;5项研究,845名参与者;中等确定性证据),并可能降低30天病死率(RR 0.68, 95% CI 0.46至1.00;3项研究,676名参与者;低确定性证据),但30天病死率的汇总ci包括无影响的可能性。开颅和血肿清除可能导致HRQoL几乎没有差异(MD 0.04, 95% CI -0.04至0.12;1项研究,445名参与者;确定性的证据)。微创手术加标准医疗管理与单独标准医疗管理相比,MIS可能增加良好功能结局的机会(RR 1.36, 95% CI 1.18至1.58;10项研究,2218名受试者;低确定性证据),并可能降低全因死亡率(RR 0.71, 95% CI 0.60 ~ 0.84;14项研究,2401名参与者;中等确定性证据)和30天病死率(RR 0.62, 95% CI 0.47至0.81;7项研究,1521名参与者;moderate-certainty证据)。HRQoL的证据非常不确定(MD -0.14, 95% CI -0.50 ~ 0.22;1项研究,27名受试者)。根据一项研究的低确定性证据,减压颅骨切除术可能增加良好功能结局的机会(RR 1.23, 95% CI 0.65 - 2)。 32;182名参与者)可能降低全因死亡率(RR 0.74, 95% CI 0.45 - 1.19;197名参与者),并可能导致HRQoL的差异很小或没有差异(MD 0.01, 95% CI -0.13至0.14),但这些结果的汇总CI包括获益和损害的可能性。减压颅骨切除术也可能降低30天病死率,但汇总CI包括无效果的可能性(RR 0.43, 95% CI 0.19至1.00;197名参与者;确定性的证据)。作者的结论是:对于自发性幕上脑出血患者,与标准医疗管理相比,旨在清除血块的手术可能增加获得良好功能结果的机会,并可能降低全因死亡率和30天病死率。当结果被血肿清除的神经外科方法划分时,开颅术可能降低全因死亡率,并可能降低30天病死率,但其对良好功能结局的影响是非常不确定的。MIS可能增加良好功能预后的机会,并可能降低全因死亡率和30天病死率。尽管对减压颅骨切除术的所有结果的效果估计可能显示有益效果,但汇总估计非常不精确,并包括有害(良好的功能结果和全因死亡率)或无效果(30天病死率)的可能性。总体而言,每种手术技术的HRQoL证据的确定性都很低或非常低。由于方法上的缺陷和大多数纳入研究的高偏倚风险,以及一些分析中不精确的汇总估计和大量异质性,证据的确定性受到限制。需要更多高质量和充分支持的研究来更加确定并指导临床实践。资金来源:Cochrane综述没有专门的资金来源。注册:协议(2022)可通过doi.org/10.1002/14651858.CD015387获得。
Surgery for spontaneous supratentorial intracerebral haemorrhage.
Rationale: It is unknown whether surgery improves outcomes in people with spontaneous supratentorial intracerebral haemorrhage (ICH), and whether the effects of surgery differ according to the applied surgical technique. This review updated the methodology of a previous Cochrane review from 2008.
Objectives: To assess the benefits and harms of surgery plus standard medical management, compared to standard medical management alone, in people with spontaneous supratentorial ICH, and to assess whether the effect of surgery differs according to the surgical technique used.
Search methods: We searched Cochrane Stroke Group Trials Register, CENTRAL, MEDLINE, and five other databases to 11 March 2025. We handsearched reference lists of included studies and relevant systematic reviews, forward-tracked relevant references, and contacted trialists for additional information on unpublished or ongoing studies.
Eligibility criteria: We included randomised controlled trials (RCTs) of surgery (craniotomy with haematoma evacuation, minimally invasive surgery (MIS), or decompressive craniectomy) plus standard medical management in adults with a spontaneous supratentorial ICH, compared with standard medical management alone. We excluded studies of people with secondary causes of ICH (such as trauma, a macrovascular cause, or an intracranial tumour).
Outcomes: Critical outcomes were: good functional outcome at end of scheduled follow-up, and all-cause mortality at end of scheduled follow-up. Important outcomes were: 30-day case fatality and health-related quality of life (HRQoL) at end of scheduled follow-up.
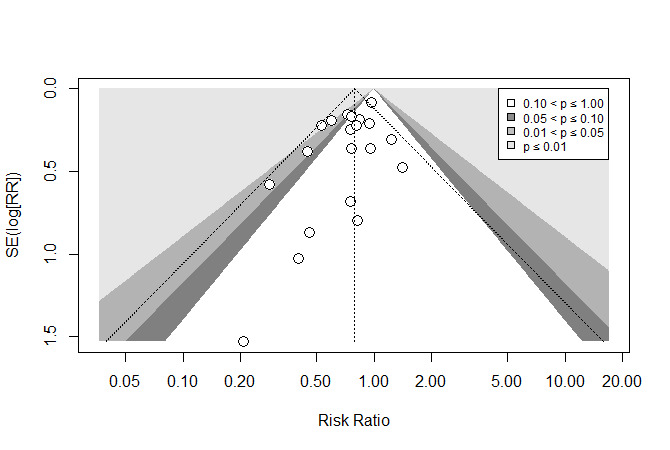
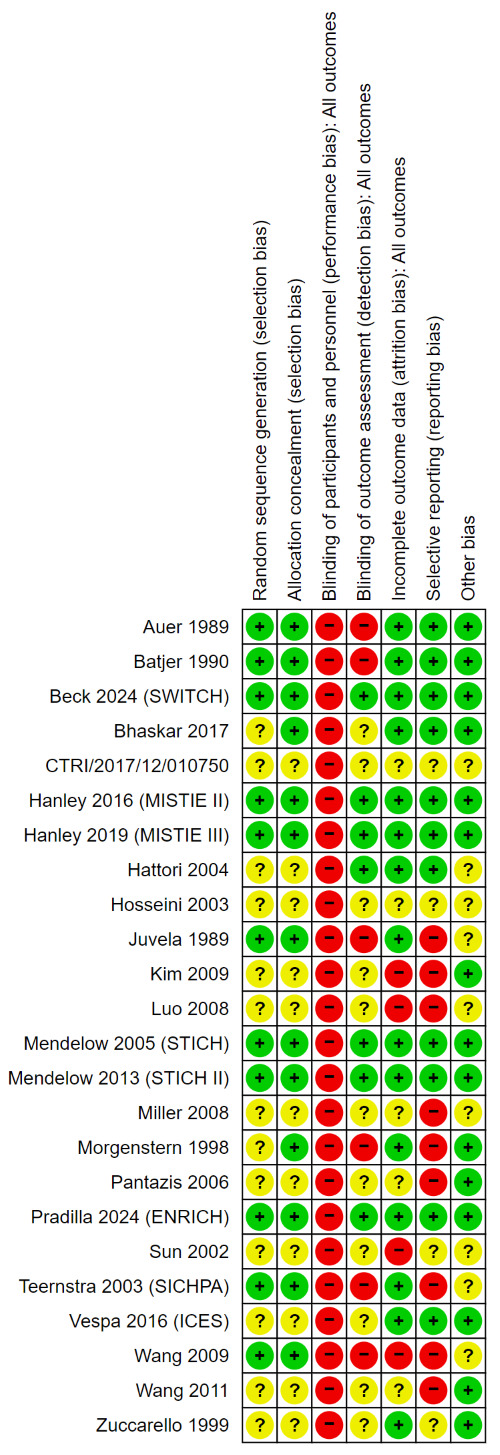
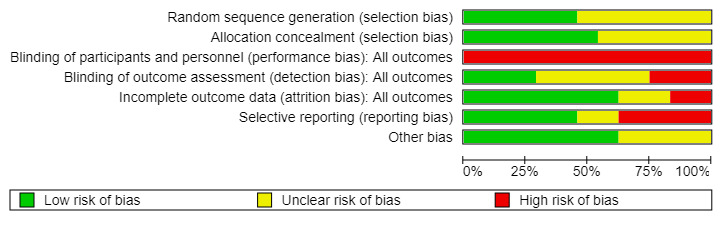
Risk of bias: We used the Cochrane RoB 1 tool.
Synthesis methods: We conducted meta-analyses using random-effects models to calculate risk ratios (RR) with 95% confidence intervals (CI) for dichotomous data, and mean differences (MD) with 95% CI for continuous data. We summarised the certainty of the evidence using GRADE.
Included studies: We included 24 RCTs (4597 participants). The studies were conducted in Europe, North and South America, Asia, Africa, and Australia, and were published between 1989 and 2024. Twenty-three studies examined surgery aimed at clot removal plus standard medical management versus standard medical management, of which six were included in the separate comparison of craniotomy with haematoma evacuation plus standard medical management versus standard medical management, and 14 in the comparison of MIS plus standard medical management versus standard medical management. One study examined decompressive craniectomy without haematoma evacuation plus standard medical management versus standard medical management.
Synthesis of results: Surgery aimed at clot removal plus standard medical management versus standard medical management alone Low-certainty evidence suggests that surgery aimed at clot removal may increase the chance of good functional outcome (RR 1.30, 95% CI 1.15 to 1.47; 18 studies, 4043 participants), and may reduce all-cause mortality (RR 0.79, 95% CI 0.71 to 0.88; 22 studies, 4278 participants) and 30-day case fatality (RR 0.74, 95% CI 0.60 to 0.90; 11 studies, 3179 participants). Surgery aimed at clot removal may have little to no effect on HRQoL, but the evidence is very uncertain (MD 0.03, 95% CI -0.05 to 0.11; 2 studies, 472 participants). Craniotomy with haematoma evacuation plus standard medical management versus standard medical management alone Craniotomy with haematoma evacuation may increase the chance of good functional outcome, but the evidence is very uncertain (RR 1.41, 95% CI 0.77 to 2.55; 6 studies, 853 participants). Craniotomy with haematoma evacuation likely reduces all-cause mortality (RR 0.80, 95% CI 0.67 to 0.96; 5 studies, 845 participants; moderate-certainty evidence), and may reduce 30-day case fatality (RR 0.68, 95% CI 0.46 to 1.00; 3 studies, 676 participants; low-certainty evidence), but the pooled CIs of 30-day case fatality included the possibility of no effect. Craniotomy with haematoma evacuation may result in little to no difference in HRQoL (MD 0.04, 95% CI -0.04 to 0.12; 1 study, 445 participants; low-certainty evidence). Minimally invasive surgery plus standard medical management versus standard medical management alone MIS may increase the chance of good functional outcome (RR 1.36, 95% CI 1.18 to 1.58; 10 studies, 2218 participants; low-certainty evidence), and probably reduces all-cause mortality (RR 0.71, 95% CI 0.60 to 0.84; 14 studies, 2401 participants; moderate-certainty evidence) and 30-day case fatality (RR 0.62, 95% CI 0.47 to 0.81; 7 studies, 1521 participants; moderate-certainty evidence). The evidence is very uncertain about HRQoL (MD -0.14, 95% CI -0.50 to 0.22; 1 study, 27 participants). Decompressive craniectomy plus standard medical management versus standard medical management alone Based on low-certainty evidence from one study, decompressive craniectomy may increase the chance of good functional outcome (RR 1.23, 95% CI 0.65 to 2.32; 182 participants), may reduce all-cause mortality (RR 0.74, 95% CI 0.45 to 1.19; 197 participants), and may result in little to no difference in HRQoL (MD 0.01, 95% CI -0.13 to 0.14), but the pooled CIs for these outcomes included the possibility of both benefit and harm. Decompressive craniectomy may also reduce 30-day case fatality, but the pooled CIs included the possibility of no effect (RR 0.43, 95% CI 0.19 to 1.00; 197 participants; low-certainty evidence).
Authors' conclusions: For people with spontaneous supratentorial ICH, surgery aimed at clot removal may increase the chance of achieving good functional outcome and may reduce all-cause mortality and 30-day case fatality compared to standard medical management. When the results are divided by neurosurgical approach for haematoma evacuation, craniotomy likely reduces all-cause mortality and may reduce 30-day case fatality, while its effect on good functional outcome is very uncertain. MIS may increase the chance of good functional outcome, and probably reduces all-cause mortality and 30-day case fatality. Although the effect estimates for all outcomes regarding decompressive craniectomy may suggest a beneficial effect, the pooled estimates were very imprecise and included the possibility of a harmful (good functional outcome and all-cause mortality) or no effect (30-day case fatality). Evidence on HRQoL was low or very low certainty, overall, and for each surgical technique. The certainty of the evidence was limited due to methodological shortcomings and the high risk of bias of most included studies, as well as imprecise pooled estimates and substantial heterogeneity in some analyses. More high-quality and adequately powered studies are needed to be more certain and to guide clinical practice.
Funding: This Cochrane review had no dedicated funding.
Registration: Protocol (2022) available via doi.org/10.1002/14651858.CD015387.
期刊介绍:
The Cochrane Database of Systematic Reviews (CDSR) stands as the premier database for systematic reviews in healthcare. It comprises Cochrane Reviews, along with protocols for these reviews, editorials, and supplements. Owned and operated by Cochrane, a worldwide independent network of healthcare stakeholders, the CDSR (ISSN 1469-493X) encompasses a broad spectrum of health-related topics, including health services.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


