Xiuzhi Jia, Wang Xiang, Huajing Peng, Jianwen Yu, Xin Wang, Hongjian Ye, Haishan Wu, Ruihan Tang, Xi Xia, Wei Chen
{"title":"用糖皮质激素单药诱导治疗I/II级狼疮性肾炎与较高的复发和较差的肾脏预后相关。","authors":"Xiuzhi Jia, Wang Xiang, Huajing Peng, Jianwen Yu, Xin Wang, Hongjian Ye, Haishan Wu, Ruihan Tang, Xi Xia, Wei Chen","doi":"10.1093/ckj/sfaf171","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The efficacy of glucocorticoid (GC) in combination with other immunosuppressive therapy for class I/II lupus nephritis (LN) remains controversial.</p><p><strong>Methods: </strong>We retrospectively analysed 107 biopsy-proven class I/II LN patients who had survival follow-up data from January 1996 to March 2023 and further assessed 96 patients with available treatment response data. These patients received GC alone (GC monotherapy) or GC in combination with another immunosuppressant (combination therapy) as induction therapy. The primary outcome was renal relapse and the secondary outcome was end-stage renal disease (ESRD) or all-cause mortality. Kaplan-Meier analysis was used to compare the cumulative renal relapse rate and long-term renal outcomes between the two treatment groups. Cox regression analysis was performed to identify the risk factors for renal relapse.</p><p><strong>Results: </strong>During a median follow-up of 112 months [interquartile range (IQR) 35.5-189.0], 96 patients had available treatment response data. All patients had complete or partial remission, with 78 (81.3%) achieving complete remission (CR). No significant difference in CR rate was observed between the GC monotherapy and combination therapy groups (82.1% versus 80.7%, <i>P</i> = .868). However, the cumulative renal relapse rate was significantly higher in the GC monotherapy group (logrank <i>P</i> = .004). GC monotherapy {hazard ratio [HR] 2.71 [95% confidence interval (CI) 1.28-5.75], <i>P</i> = .009} and partial remission after induction therapy [HR 4.17 (95% CI 1.78-9.80), <i>P</i> = .001] were independent risk factors for renal relapse. After a median follow-up time of 156 months (IQR 76.0-199.0), four patients (3.7%) developed ESRD, all in the GC monotherapy group. Long-term renal outcome in the GC monotherapy group was significantly poorer, with 5-, 10-, 15- and 20-year renal survival rates of 100.0%, 93.9%, 90.4% and 90.4%, respectively (<i>P</i> = .025).</p><p><strong>Conclusion: </strong>Class I/II LN patients treated with GC monotherapy have higher renal relapse rates and poorer long-term renal outcomes compared with those receiving GC in combination with other immunosuppressants as induction therapy.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 7","pages":"sfaf171"},"PeriodicalIF":4.6000,"publicationDate":"2025-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12264484/pdf/","citationCount":"0","resultStr":"{\"title\":\"Induction therapy for class I/II lupus nephritis with glucocorticoid monotherapy associates with higher relapse and poorer kidney outcomes.\",\"authors\":\"Xiuzhi Jia, Wang Xiang, Huajing Peng, Jianwen Yu, Xin Wang, Hongjian Ye, Haishan Wu, Ruihan Tang, Xi Xia, Wei Chen\",\"doi\":\"10.1093/ckj/sfaf171\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The efficacy of glucocorticoid (GC) in combination with other immunosuppressive therapy for class I/II lupus nephritis (LN) remains controversial.</p><p><strong>Methods: </strong>We retrospectively analysed 107 biopsy-proven class I/II LN patients who had survival follow-up data from January 1996 to March 2023 and further assessed 96 patients with available treatment response data. These patients received GC alone (GC monotherapy) or GC in combination with another immunosuppressant (combination therapy) as induction therapy. The primary outcome was renal relapse and the secondary outcome was end-stage renal disease (ESRD) or all-cause mortality. Kaplan-Meier analysis was used to compare the cumulative renal relapse rate and long-term renal outcomes between the two treatment groups. Cox regression analysis was performed to identify the risk factors for renal relapse.</p><p><strong>Results: </strong>During a median follow-up of 112 months [interquartile range (IQR) 35.5-189.0], 96 patients had available treatment response data. All patients had complete or partial remission, with 78 (81.3%) achieving complete remission (CR). No significant difference in CR rate was observed between the GC monotherapy and combination therapy groups (82.1% versus 80.7%, <i>P</i> = .868). However, the cumulative renal relapse rate was significantly higher in the GC monotherapy group (logrank <i>P</i> = .004). GC monotherapy {hazard ratio [HR] 2.71 [95% confidence interval (CI) 1.28-5.75], <i>P</i> = .009} and partial remission after induction therapy [HR 4.17 (95% CI 1.78-9.80), <i>P</i> = .001] were independent risk factors for renal relapse. After a median follow-up time of 156 months (IQR 76.0-199.0), four patients (3.7%) developed ESRD, all in the GC monotherapy group. Long-term renal outcome in the GC monotherapy group was significantly poorer, with 5-, 10-, 15- and 20-year renal survival rates of 100.0%, 93.9%, 90.4% and 90.4%, respectively (<i>P</i> = .025).</p><p><strong>Conclusion: </strong>Class I/II LN patients treated with GC monotherapy have higher renal relapse rates and poorer long-term renal outcomes compared with those receiving GC in combination with other immunosuppressants as induction therapy.</p>\",\"PeriodicalId\":10435,\"journal\":{\"name\":\"Clinical Kidney Journal\",\"volume\":\"18 7\",\"pages\":\"sfaf171\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2025-07-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12264484/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Kidney Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ckj/sfaf171\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf171","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:糖皮质激素(GC)联合其他免疫抑制疗法治疗I/II型狼疮性肾炎(LN)的疗效仍存在争议。方法:我们回顾性分析了107例活检证实的I/II级LN患者,这些患者从1996年1月到2023年3月有生存随访数据,并进一步评估了96例患者的可用治疗反应数据。这些患者接受单独GC (GC单药治疗)或GC联合另一种免疫抑制剂(联合治疗)作为诱导治疗。主要结局是肾脏复发,次要结局是终末期肾脏疾病(ESRD)或全因死亡率。Kaplan-Meier分析比较两组患者肾脏累积复发率和长期预后。采用Cox回归分析确定肾脏复发的危险因素。结果:中位随访时间为112个月[四分位间距(IQR) 35.5-189.0], 96例患者可获得治疗反应数据。所有患者均有完全或部分缓解,其中78例(81.3%)达到完全缓解(CR)。GC单药组与联合治疗组CR率无显著差异(82.1% vs 80.7%, P = 0.868)。然而,GC单药治疗组的累计肾脏复发率明显高于对照组(洛格兰P = 0.004)。GC单药治疗{危险比[HR] 2.71[95%可信区间(CI) 1.28 ~ 5.75], P = 0.009}和诱导治疗后部分缓解[HR 4.17 (95% CI 1.78 ~ 9.80), P = 0.001]是肾脏复发的独立危险因素。中位随访156个月(IQR 76.0-199.0), 4例(3.7%)发生ESRD,均为GC单药治疗组。GC单药组长期肾脏预后明显较差,5年、10年、15年和20年肾脏生存率分别为100.0%、93.9%、90.4%和90.4% (P = 0.025)。结论:与GC联合其他免疫抑制剂诱导治疗相比,GC单药治疗的I/II级LN患者有更高的肾脏复发率和更差的长期肾脏预后。
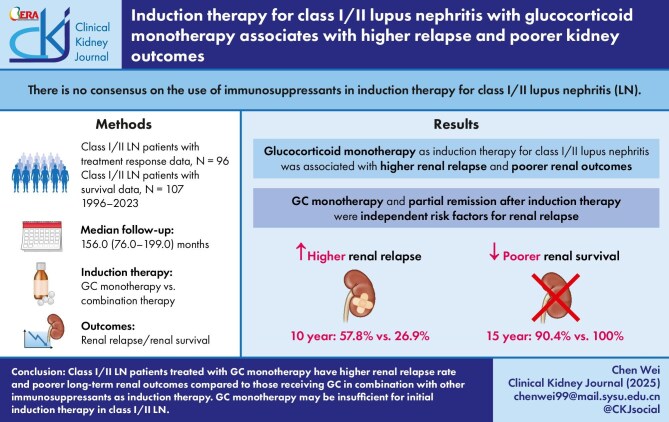
Induction therapy for class I/II lupus nephritis with glucocorticoid monotherapy associates with higher relapse and poorer kidney outcomes.
Background: The efficacy of glucocorticoid (GC) in combination with other immunosuppressive therapy for class I/II lupus nephritis (LN) remains controversial.
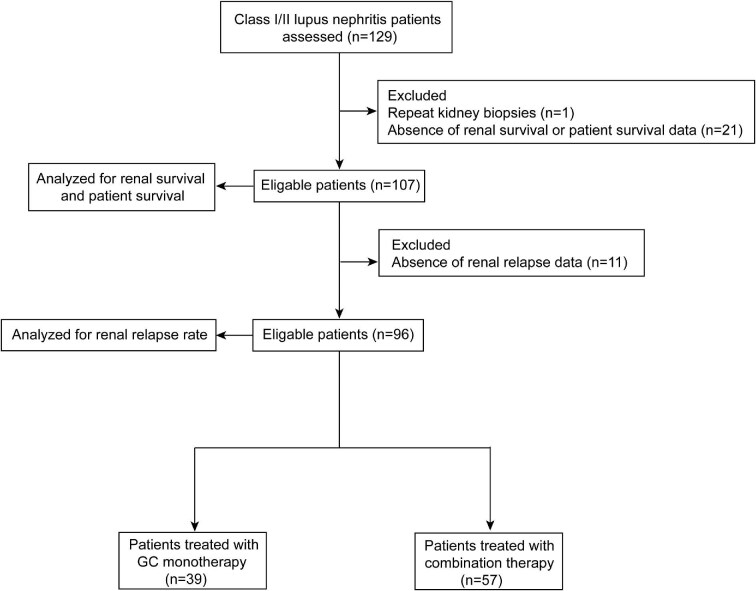
Methods: We retrospectively analysed 107 biopsy-proven class I/II LN patients who had survival follow-up data from January 1996 to March 2023 and further assessed 96 patients with available treatment response data. These patients received GC alone (GC monotherapy) or GC in combination with another immunosuppressant (combination therapy) as induction therapy. The primary outcome was renal relapse and the secondary outcome was end-stage renal disease (ESRD) or all-cause mortality. Kaplan-Meier analysis was used to compare the cumulative renal relapse rate and long-term renal outcomes between the two treatment groups. Cox regression analysis was performed to identify the risk factors for renal relapse.
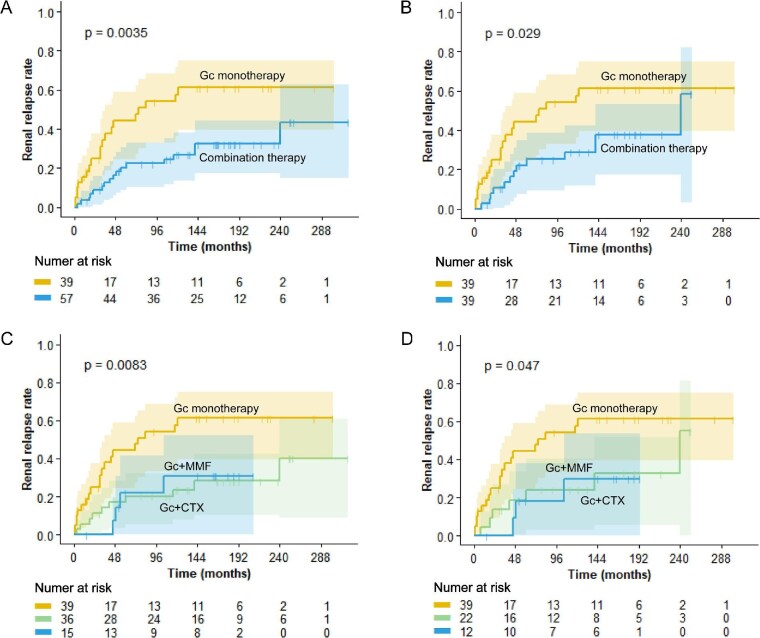
Results: During a median follow-up of 112 months [interquartile range (IQR) 35.5-189.0], 96 patients had available treatment response data. All patients had complete or partial remission, with 78 (81.3%) achieving complete remission (CR). No significant difference in CR rate was observed between the GC monotherapy and combination therapy groups (82.1% versus 80.7%, P = .868). However, the cumulative renal relapse rate was significantly higher in the GC monotherapy group (logrank P = .004). GC monotherapy {hazard ratio [HR] 2.71 [95% confidence interval (CI) 1.28-5.75], P = .009} and partial remission after induction therapy [HR 4.17 (95% CI 1.78-9.80), P = .001] were independent risk factors for renal relapse. After a median follow-up time of 156 months (IQR 76.0-199.0), four patients (3.7%) developed ESRD, all in the GC monotherapy group. Long-term renal outcome in the GC monotherapy group was significantly poorer, with 5-, 10-, 15- and 20-year renal survival rates of 100.0%, 93.9%, 90.4% and 90.4%, respectively (P = .025).
Conclusion: Class I/II LN patients treated with GC monotherapy have higher renal relapse rates and poorer long-term renal outcomes compared with those receiving GC in combination with other immunosuppressants as induction therapy.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


