{"title":"院级门到体外心肺复苏中位时间对难治性院外心脏骤停患者预后的影响","authors":"Daisuke Kasugai, Yohei Okada, Yuka Mizutani, Junta Honda, Toru Kondo, Shingo Kazama, Takanori Yamamoto","doi":"10.1097/CCM.0000000000006808","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the impact of hospital-level median door-to-extracorporeal cardiopulmonary resuscitation (ECPR) time on survival and neurologic outcomes in patients with out-of-hospital cardiac arrest (OHCA) requiring ECPR.</p><p><strong>Design: </strong>Secondary analysis of the Japanese Association for Acute Medicine OHCA registry, a nationwide Japanese database of OHCA patients.</p><p><strong>Setting: </strong>Fifty-three hospitals across Japan.</p><p><strong>Patients: </strong>Adult patients who underwent ECPR between 2014 and 2021 were included. Hospitals were categorized into \"rapid\" or \"delayed\" groups based on their median door-to-ECPR times.</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>The primary outcome was 30-day survival. Secondary outcomes included 30-day and 90-day survival with favorable neurologic outcomes. Propensity score weighting was applied to adjust for confounders. In total, 2136 patients treated at 53 hospitals were included. Hospitals with shorter median door-to-ECPR times had higher 30-day survival rates (odds ratio [OR], 1.36; 95% CI, 1.21-1.53). Neurologic outcomes were better in the rapid hospital group at both 30 days (OR, 1.47; 95% CI, 1.24-1.73) and 90 days (OR, 1.47; 95% CI, 1.25-1.73) follow-ups.</p><p><strong>Conclusions: </strong>Hospital-level median door-to-ECPR time is a crucial predictor of survival and neurologic outcomes in OHCA patients requiring ECPR. Shorter door-to-ECPR times should be considered a key quality metric for ECPR processes.</p>","PeriodicalId":10765,"journal":{"name":"Critical Care Medicine","volume":" ","pages":"e2025-e2032"},"PeriodicalIF":6.0000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12490338/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Impact of Hospital-Level Median Door-to-Extracorporeal Cardiopulmonary Resuscitation Time on the Prognosis of Patients With Refractory Out-of-Hospital Cardiac Arrest.\",\"authors\":\"Daisuke Kasugai, Yohei Okada, Yuka Mizutani, Junta Honda, Toru Kondo, Shingo Kazama, Takanori Yamamoto\",\"doi\":\"10.1097/CCM.0000000000006808\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To evaluate the impact of hospital-level median door-to-extracorporeal cardiopulmonary resuscitation (ECPR) time on survival and neurologic outcomes in patients with out-of-hospital cardiac arrest (OHCA) requiring ECPR.</p><p><strong>Design: </strong>Secondary analysis of the Japanese Association for Acute Medicine OHCA registry, a nationwide Japanese database of OHCA patients.</p><p><strong>Setting: </strong>Fifty-three hospitals across Japan.</p><p><strong>Patients: </strong>Adult patients who underwent ECPR between 2014 and 2021 were included. Hospitals were categorized into \\\"rapid\\\" or \\\"delayed\\\" groups based on their median door-to-ECPR times.</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>The primary outcome was 30-day survival. Secondary outcomes included 30-day and 90-day survival with favorable neurologic outcomes. Propensity score weighting was applied to adjust for confounders. In total, 2136 patients treated at 53 hospitals were included. Hospitals with shorter median door-to-ECPR times had higher 30-day survival rates (odds ratio [OR], 1.36; 95% CI, 1.21-1.53). Neurologic outcomes were better in the rapid hospital group at both 30 days (OR, 1.47; 95% CI, 1.24-1.73) and 90 days (OR, 1.47; 95% CI, 1.25-1.73) follow-ups.</p><p><strong>Conclusions: </strong>Hospital-level median door-to-ECPR time is a crucial predictor of survival and neurologic outcomes in OHCA patients requiring ECPR. Shorter door-to-ECPR times should be considered a key quality metric for ECPR processes.</p>\",\"PeriodicalId\":10765,\"journal\":{\"name\":\"Critical Care Medicine\",\"volume\":\" \",\"pages\":\"e2025-e2032\"},\"PeriodicalIF\":6.0000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12490338/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/CCM.0000000000006808\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/CCM.0000000000006808","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/16 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
The Impact of Hospital-Level Median Door-to-Extracorporeal Cardiopulmonary Resuscitation Time on the Prognosis of Patients With Refractory Out-of-Hospital Cardiac Arrest.
Objectives: To evaluate the impact of hospital-level median door-to-extracorporeal cardiopulmonary resuscitation (ECPR) time on survival and neurologic outcomes in patients with out-of-hospital cardiac arrest (OHCA) requiring ECPR.
Design: Secondary analysis of the Japanese Association for Acute Medicine OHCA registry, a nationwide Japanese database of OHCA patients.
Setting: Fifty-three hospitals across Japan.
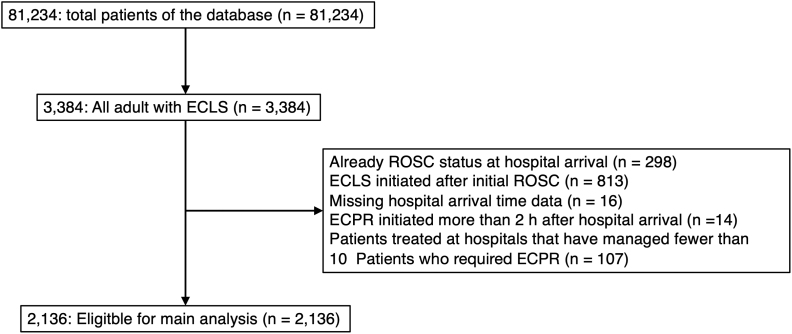
Patients: Adult patients who underwent ECPR between 2014 and 2021 were included. Hospitals were categorized into "rapid" or "delayed" groups based on their median door-to-ECPR times.
Interventions: None.
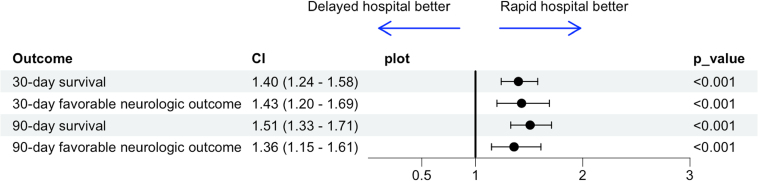
Measurements and main results: The primary outcome was 30-day survival. Secondary outcomes included 30-day and 90-day survival with favorable neurologic outcomes. Propensity score weighting was applied to adjust for confounders. In total, 2136 patients treated at 53 hospitals were included. Hospitals with shorter median door-to-ECPR times had higher 30-day survival rates (odds ratio [OR], 1.36; 95% CI, 1.21-1.53). Neurologic outcomes were better in the rapid hospital group at both 30 days (OR, 1.47; 95% CI, 1.24-1.73) and 90 days (OR, 1.47; 95% CI, 1.25-1.73) follow-ups.
Conclusions: Hospital-level median door-to-ECPR time is a crucial predictor of survival and neurologic outcomes in OHCA patients requiring ECPR. Shorter door-to-ECPR times should be considered a key quality metric for ECPR processes.
期刊介绍:
Critical Care Medicine is the premier peer-reviewed, scientific publication in critical care medicine. Directed to those specialists who treat patients in the ICU and CCU, including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals, Critical Care Medicine covers all aspects of acute and emergency care for the critically ill or injured patient.
Each issue presents critical care practitioners with clinical breakthroughs that lead to better patient care, the latest news on promising research, and advances in equipment and techniques.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


