Stepan Havranek, Jakub Neuhöfer, Michaela Vesela, Petra Kavalkova, Daniel Rob, Zdenka Fingrova, Jana Smalcova, Ondrej Franek, Michal Huptych, Milan Dusik, Jan Pudil, Vojtech Weiss, Ales Linhart, Jan Belohlavek
{"title":"难治性院外心脏骤停的心律转换和结果:体外复苏与常规复苏。","authors":"Stepan Havranek, Jakub Neuhöfer, Michaela Vesela, Petra Kavalkova, Daniel Rob, Zdenka Fingrova, Jana Smalcova, Ondrej Franek, Michal Huptych, Milan Dusik, Jan Pudil, Vojtech Weiss, Ales Linhart, Jan Belohlavek","doi":"10.1097/CCM.0000000000006787","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>A Prague out-of-hospital cardiac arrest (OHCA) study has demonstrated that an invasive approach (early transport to the hospital, extracorporeal cardiopulmonary resuscitation [ECPR]) is a feasible and effective treatment strategy in refractory OHCA. This post hoc analysis of the Prague OHCA study aimed to stratify the prognosis of patients according to the detailed course of heart rhythm during prehospital and early hospital periods.</p><p><strong>Design, setting, and patients: </strong>This analysis included all 256 patients (median age 58, 17% females) randomized to the Prague OHCA study. The sequence of heart rhythms during the prehospital period was analyzed in terms of neurologic outcomes after 180 days. The primary outcome was a composite of survival with Cerebral Performance Category 1 or 2 at 180 days.</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>Within the study cohort, 156 (61%) manifested ventricular fibrillation (VF), 45 pulseless electrical activity, and 55 asystole as the initial rhythm. Patients with an initial VF who reached a sustained recovery of spontaneous circulation (ROSC) had the highest proportion of reaching a primary outcome (32/44 [73%]). Patients who had one or more episodes of asystole during cardiopulmonary resuscitation had the lowest rate of primary endpoint (5/39 [13%]). Patients who experienced intermittent ROSC showed a higher success rate in achieving the primary outcome when treated with an invasive-based approach (including ECPR) compared with the conventional strategy (26/34 [76%] vs. 24/50 [48%]; p < 0.05).</p><p><strong>Conclusions: </strong>Achieving ROSC is the best prognostic marker in OHCA patients with an initially refractory VF. Patients with intermittent ROSC after the initial VF and ongoing VF seem to be optimal candidates for an invasive approach. Asystole detection at any time during resuscitation is a strong negative prognostic marker, irrespective of the initial rhythm.</p>","PeriodicalId":10765,"journal":{"name":"Critical Care Medicine","volume":" ","pages":"e1930-e1940"},"PeriodicalIF":6.0000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12490342/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cardiac Rhythm Conversions and the Outcome in Refractory Out-of-Hospital Cardiac Arrest: Extracorporeal Versus Conventional Resuscitation.\",\"authors\":\"Stepan Havranek, Jakub Neuhöfer, Michaela Vesela, Petra Kavalkova, Daniel Rob, Zdenka Fingrova, Jana Smalcova, Ondrej Franek, Michal Huptych, Milan Dusik, Jan Pudil, Vojtech Weiss, Ales Linhart, Jan Belohlavek\",\"doi\":\"10.1097/CCM.0000000000006787\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>A Prague out-of-hospital cardiac arrest (OHCA) study has demonstrated that an invasive approach (early transport to the hospital, extracorporeal cardiopulmonary resuscitation [ECPR]) is a feasible and effective treatment strategy in refractory OHCA. This post hoc analysis of the Prague OHCA study aimed to stratify the prognosis of patients according to the detailed course of heart rhythm during prehospital and early hospital periods.</p><p><strong>Design, setting, and patients: </strong>This analysis included all 256 patients (median age 58, 17% females) randomized to the Prague OHCA study. The sequence of heart rhythms during the prehospital period was analyzed in terms of neurologic outcomes after 180 days. The primary outcome was a composite of survival with Cerebral Performance Category 1 or 2 at 180 days.</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>Within the study cohort, 156 (61%) manifested ventricular fibrillation (VF), 45 pulseless electrical activity, and 55 asystole as the initial rhythm. Patients with an initial VF who reached a sustained recovery of spontaneous circulation (ROSC) had the highest proportion of reaching a primary outcome (32/44 [73%]). Patients who had one or more episodes of asystole during cardiopulmonary resuscitation had the lowest rate of primary endpoint (5/39 [13%]). Patients who experienced intermittent ROSC showed a higher success rate in achieving the primary outcome when treated with an invasive-based approach (including ECPR) compared with the conventional strategy (26/34 [76%] vs. 24/50 [48%]; p < 0.05).</p><p><strong>Conclusions: </strong>Achieving ROSC is the best prognostic marker in OHCA patients with an initially refractory VF. Patients with intermittent ROSC after the initial VF and ongoing VF seem to be optimal candidates for an invasive approach. Asystole detection at any time during resuscitation is a strong negative prognostic marker, irrespective of the initial rhythm.</p>\",\"PeriodicalId\":10765,\"journal\":{\"name\":\"Critical Care Medicine\",\"volume\":\" \",\"pages\":\"e1930-e1940\"},\"PeriodicalIF\":6.0000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12490342/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/CCM.0000000000006787\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/CCM.0000000000006787","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/16 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Cardiac Rhythm Conversions and the Outcome in Refractory Out-of-Hospital Cardiac Arrest: Extracorporeal Versus Conventional Resuscitation.
Objectives: A Prague out-of-hospital cardiac arrest (OHCA) study has demonstrated that an invasive approach (early transport to the hospital, extracorporeal cardiopulmonary resuscitation [ECPR]) is a feasible and effective treatment strategy in refractory OHCA. This post hoc analysis of the Prague OHCA study aimed to stratify the prognosis of patients according to the detailed course of heart rhythm during prehospital and early hospital periods.
Design, setting, and patients: This analysis included all 256 patients (median age 58, 17% females) randomized to the Prague OHCA study. The sequence of heart rhythms during the prehospital period was analyzed in terms of neurologic outcomes after 180 days. The primary outcome was a composite of survival with Cerebral Performance Category 1 or 2 at 180 days.
Interventions: None.
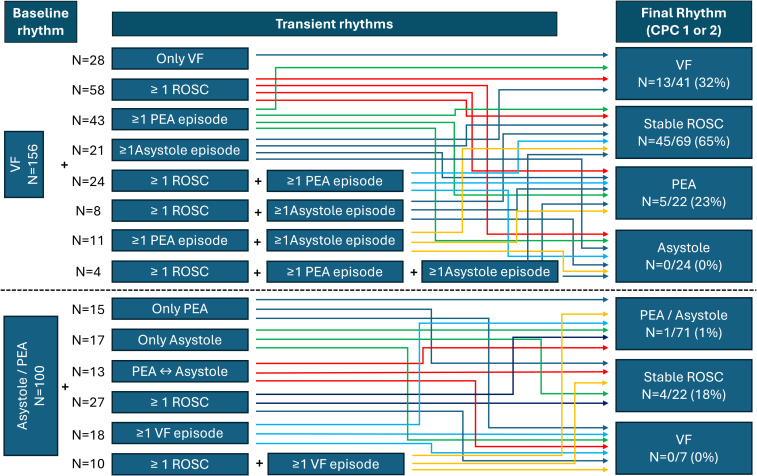
Measurements and main results: Within the study cohort, 156 (61%) manifested ventricular fibrillation (VF), 45 pulseless electrical activity, and 55 asystole as the initial rhythm. Patients with an initial VF who reached a sustained recovery of spontaneous circulation (ROSC) had the highest proportion of reaching a primary outcome (32/44 [73%]). Patients who had one or more episodes of asystole during cardiopulmonary resuscitation had the lowest rate of primary endpoint (5/39 [13%]). Patients who experienced intermittent ROSC showed a higher success rate in achieving the primary outcome when treated with an invasive-based approach (including ECPR) compared with the conventional strategy (26/34 [76%] vs. 24/50 [48%]; p < 0.05).
Conclusions: Achieving ROSC is the best prognostic marker in OHCA patients with an initially refractory VF. Patients with intermittent ROSC after the initial VF and ongoing VF seem to be optimal candidates for an invasive approach. Asystole detection at any time during resuscitation is a strong negative prognostic marker, irrespective of the initial rhythm.
期刊介绍:
Critical Care Medicine is the premier peer-reviewed, scientific publication in critical care medicine. Directed to those specialists who treat patients in the ICU and CCU, including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals, Critical Care Medicine covers all aspects of acute and emergency care for the critically ill or injured patient.
Each issue presents critical care practitioners with clinical breakthroughs that lead to better patient care, the latest news on promising research, and advances in equipment and techniques.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


