Marco Juul Thomsen, Stine Linding Andersen, Nanna Maria Uldall Torp, Stig Andersen, Allan Carlé
{"title":"联合免疫检查点抑制剂治疗后甲状腺功能障碍亚型疾病实体的挑战:一个病例报告。","authors":"Marco Juul Thomsen, Stine Linding Andersen, Nanna Maria Uldall Torp, Stig Andersen, Allan Carlé","doi":"10.1186/s13044-025-00254-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Immune checkpoint inhibitor (ICI) therapy is used in the management of advanced malignancies. Thyroid function abnormalities have been reported, but more evidence is needed to substantiate the subtypes and course of thyroid disease associated with this treatment.</p><p><strong>Case presentation: </strong>A 51-year-old woman with metastatic pancreatic cancer and no previous history of autoimmune disease was referred to the Endocrine Department six days after the initiation of combined treatment with ipilimumab (anti-CTLA-4) and nivolumab (anti-PD-1). At the initial endocrinologic assessment, the patient had biochemical overt thyrotoxicosis with suppressed thyroid stimulating hormone < 0.01 mIU/L (reference range (RR), 0.3-4.5 mIU/L), elevated total thyroxine (TT4) > 309 nmol/L (> 24.0 µg/dL) (RR, 60-140 nmol/L; 4.7-10.9 µg/dL), and total triiodothyronine (TT3) 7.0 nmol/L (454.5 ng/dL) (RR, 1.1-2.5 nmol/L; 71.4-162.3 ng/dL). Despite marked biochemical thyrotoxicosis, the patient presented with few symptoms. TSH-receptor antibodies (TRAb) were negative, as were thyroid peroxidase antibodies, whereas elevated levels of thyroglobulin antibodies were found. Thyroid ultrasound revealed an enlarged, heterogeneous hypoechoic gland with increased vascularity. High-dose antithyroid drug (ATD) therapy were followed by a decline in thyroid hormone levels (after one week of treatment: TT4: >309 nmol/L (> 24.0 µg/dL); TT3: 1.8 nmol/L (116.9 ng/dL); after two weeks: TT4: 164 nmol/L (12.7 µg/dL); TT3: 0.9 nmol/L (58.4 ng/dL)). After five weeks, the patient developed biochemical hypothyroidism. Thus, ATD therapy was discontinued, and levothyroxine was initiated.</p><p><strong>Conclusion: </strong>This case report illustrates with a short time frame from the initiation of ICI therapy the onset of thyrotoxicosis, followed by the development of thyroid insufficiency. This case highlights the challenges associated with subtyping the cause of thyroid dysfunction in patients treated with ICIs. Further, this case highlights the importance of clinical awareness and close monitoring of thyroid function in patients receiving immunotherapy.</p>","PeriodicalId":39048,"journal":{"name":"Thyroid Research","volume":"18 1","pages":"35"},"PeriodicalIF":1.8000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12261766/pdf/","citationCount":"0","resultStr":"{\"title\":\"Challenges in subtyping disease entities of thyroid dysfunction following combined immune checkpoint inhibitor therapy: a case report.\",\"authors\":\"Marco Juul Thomsen, Stine Linding Andersen, Nanna Maria Uldall Torp, Stig Andersen, Allan Carlé\",\"doi\":\"10.1186/s13044-025-00254-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Immune checkpoint inhibitor (ICI) therapy is used in the management of advanced malignancies. Thyroid function abnormalities have been reported, but more evidence is needed to substantiate the subtypes and course of thyroid disease associated with this treatment.</p><p><strong>Case presentation: </strong>A 51-year-old woman with metastatic pancreatic cancer and no previous history of autoimmune disease was referred to the Endocrine Department six days after the initiation of combined treatment with ipilimumab (anti-CTLA-4) and nivolumab (anti-PD-1). At the initial endocrinologic assessment, the patient had biochemical overt thyrotoxicosis with suppressed thyroid stimulating hormone < 0.01 mIU/L (reference range (RR), 0.3-4.5 mIU/L), elevated total thyroxine (TT4) > 309 nmol/L (> 24.0 µg/dL) (RR, 60-140 nmol/L; 4.7-10.9 µg/dL), and total triiodothyronine (TT3) 7.0 nmol/L (454.5 ng/dL) (RR, 1.1-2.5 nmol/L; 71.4-162.3 ng/dL). Despite marked biochemical thyrotoxicosis, the patient presented with few symptoms. TSH-receptor antibodies (TRAb) were negative, as were thyroid peroxidase antibodies, whereas elevated levels of thyroglobulin antibodies were found. Thyroid ultrasound revealed an enlarged, heterogeneous hypoechoic gland with increased vascularity. High-dose antithyroid drug (ATD) therapy were followed by a decline in thyroid hormone levels (after one week of treatment: TT4: >309 nmol/L (> 24.0 µg/dL); TT3: 1.8 nmol/L (116.9 ng/dL); after two weeks: TT4: 164 nmol/L (12.7 µg/dL); TT3: 0.9 nmol/L (58.4 ng/dL)). After five weeks, the patient developed biochemical hypothyroidism. Thus, ATD therapy was discontinued, and levothyroxine was initiated.</p><p><strong>Conclusion: </strong>This case report illustrates with a short time frame from the initiation of ICI therapy the onset of thyrotoxicosis, followed by the development of thyroid insufficiency. This case highlights the challenges associated with subtyping the cause of thyroid dysfunction in patients treated with ICIs. Further, this case highlights the importance of clinical awareness and close monitoring of thyroid function in patients receiving immunotherapy.</p>\",\"PeriodicalId\":39048,\"journal\":{\"name\":\"Thyroid Research\",\"volume\":\"18 1\",\"pages\":\"35\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12261766/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Thyroid Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13044-025-00254-7\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thyroid Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13044-025-00254-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Challenges in subtyping disease entities of thyroid dysfunction following combined immune checkpoint inhibitor therapy: a case report.
Background: Immune checkpoint inhibitor (ICI) therapy is used in the management of advanced malignancies. Thyroid function abnormalities have been reported, but more evidence is needed to substantiate the subtypes and course of thyroid disease associated with this treatment.
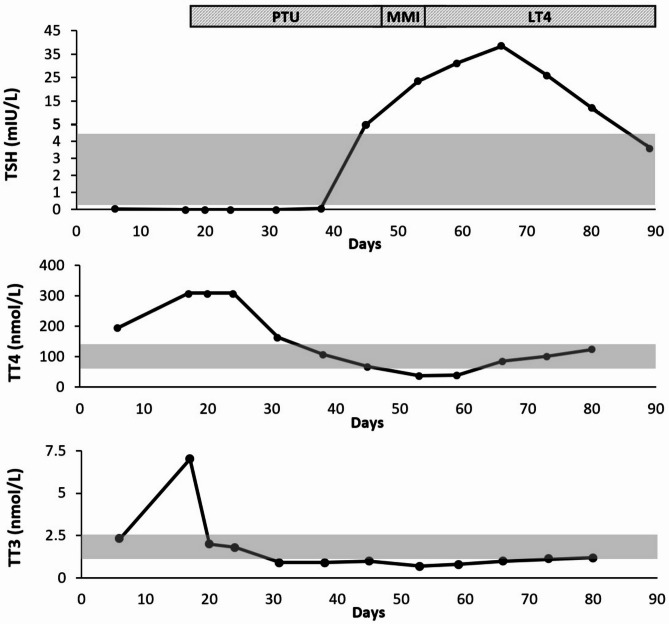
Case presentation: A 51-year-old woman with metastatic pancreatic cancer and no previous history of autoimmune disease was referred to the Endocrine Department six days after the initiation of combined treatment with ipilimumab (anti-CTLA-4) and nivolumab (anti-PD-1). At the initial endocrinologic assessment, the patient had biochemical overt thyrotoxicosis with suppressed thyroid stimulating hormone < 0.01 mIU/L (reference range (RR), 0.3-4.5 mIU/L), elevated total thyroxine (TT4) > 309 nmol/L (> 24.0 µg/dL) (RR, 60-140 nmol/L; 4.7-10.9 µg/dL), and total triiodothyronine (TT3) 7.0 nmol/L (454.5 ng/dL) (RR, 1.1-2.5 nmol/L; 71.4-162.3 ng/dL). Despite marked biochemical thyrotoxicosis, the patient presented with few symptoms. TSH-receptor antibodies (TRAb) were negative, as were thyroid peroxidase antibodies, whereas elevated levels of thyroglobulin antibodies were found. Thyroid ultrasound revealed an enlarged, heterogeneous hypoechoic gland with increased vascularity. High-dose antithyroid drug (ATD) therapy were followed by a decline in thyroid hormone levels (after one week of treatment: TT4: >309 nmol/L (> 24.0 µg/dL); TT3: 1.8 nmol/L (116.9 ng/dL); after two weeks: TT4: 164 nmol/L (12.7 µg/dL); TT3: 0.9 nmol/L (58.4 ng/dL)). After five weeks, the patient developed biochemical hypothyroidism. Thus, ATD therapy was discontinued, and levothyroxine was initiated.
Conclusion: This case report illustrates with a short time frame from the initiation of ICI therapy the onset of thyrotoxicosis, followed by the development of thyroid insufficiency. This case highlights the challenges associated with subtyping the cause of thyroid dysfunction in patients treated with ICIs. Further, this case highlights the importance of clinical awareness and close monitoring of thyroid function in patients receiving immunotherapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


