Bedreddin Kalyenci, Ferhat Çoban, Hasan Sulhan, Mehmet Özgür Yücel, Can Benlioğlu, Gazi Kaz, Tayfun Şahinkanat, Ali Çift
{"title":"泛免疫炎症值和全身免疫炎症指数作为预测逆行肾内手术后感染并发症的潜在生物标志物的作用","authors":"Bedreddin Kalyenci, Ferhat Çoban, Hasan Sulhan, Mehmet Özgür Yücel, Can Benlioğlu, Gazi Kaz, Tayfun Şahinkanat, Ali Çift","doi":"10.1186/s12894-025-01859-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To predict postoperative infectious complications by utilizing hemogram parameters and derived inflammation indices and to analyze patient-related risk factors to propose a nomogram.</p><p><strong>Methods: </strong>The data of patients who underwent retrograde intrarenal surgery were reviewed. The patients were categorized into two groups: those without infectious complications (Group A) and those with infectious complications (Group B). Infectious complications were defined as fever persisting above 38 °C for 48 h and the presence of two or more systemic inflammatory response syndrome (SIRS) criteria. Hemogram parameters and inflammation indices were examined to predict infectious complications. The study utilized neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR), along with the pan-immune-inflammation value (PIV) and systemic immune-inflammation index (SII).</p><p><strong>Results: </strong>The data of 658 cases were evaluated. No infectious complications were observed in 610 cases (92.7%), while 33 cases (5.0%) developed fever, and 15 cases (2.3%) met the criteria for SIRS. The optimal cut-off values for distinguishing between groups were determined as follows: >2.66 for NLR, > 122.5 for PLR, < 2.81 for LMR, > 619.4 for SII, and > 500.2 for PIV. Patients with PIV > 500.2 exhibited a 13.737-fold increase (95% confidence interval [CI]: 7.260-25.994) in infectious complications compared to those with PIV ≤ 500.2, making PIV the strongest predictor. The most significant factors in differentiating between the groups were, in order of importance, Charlson comorbidity index, stone volume, preoperative serum creatinine level, and preoperative double-J stent placement. These factors were analyzed using multivariate logistic regression alongside PIV and SII, and two models were constructed. The predictive power of Model 1 was determined as Cox & Snell R² = 0.269 and Nagelkerke R² = 0.661, while Model 2 had a Cox & Snell R² value of 0.264 and a Nagelkerke R² value of 0.648.</p><p><strong>Conclusion: </strong>PIV and SII, derived from hemogram parameters, serve as predictive inflammatory indices for postoperative infectious complications. They provide valuable preoperative insight into the patient's immune and systemic inflammatory responses. When combined with other risk factors, these indices allow for the prediction of postoperative infectious complications.</p>","PeriodicalId":9285,"journal":{"name":"BMC Urology","volume":"25 1","pages":"168"},"PeriodicalIF":1.9000,"publicationDate":"2025-07-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12257762/pdf/","citationCount":"0","resultStr":"{\"title\":\"The role of Pan-Immune inflammation value and systemic Immune-Inflammation index as potential biomarkers in predicting infectious complications following retrograde intrarenal surgery.\",\"authors\":\"Bedreddin Kalyenci, Ferhat Çoban, Hasan Sulhan, Mehmet Özgür Yücel, Can Benlioğlu, Gazi Kaz, Tayfun Şahinkanat, Ali Çift\",\"doi\":\"10.1186/s12894-025-01859-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>To predict postoperative infectious complications by utilizing hemogram parameters and derived inflammation indices and to analyze patient-related risk factors to propose a nomogram.</p><p><strong>Methods: </strong>The data of patients who underwent retrograde intrarenal surgery were reviewed. The patients were categorized into two groups: those without infectious complications (Group A) and those with infectious complications (Group B). Infectious complications were defined as fever persisting above 38 °C for 48 h and the presence of two or more systemic inflammatory response syndrome (SIRS) criteria. Hemogram parameters and inflammation indices were examined to predict infectious complications. The study utilized neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR), along with the pan-immune-inflammation value (PIV) and systemic immune-inflammation index (SII).</p><p><strong>Results: </strong>The data of 658 cases were evaluated. No infectious complications were observed in 610 cases (92.7%), while 33 cases (5.0%) developed fever, and 15 cases (2.3%) met the criteria for SIRS. The optimal cut-off values for distinguishing between groups were determined as follows: >2.66 for NLR, > 122.5 for PLR, < 2.81 for LMR, > 619.4 for SII, and > 500.2 for PIV. Patients with PIV > 500.2 exhibited a 13.737-fold increase (95% confidence interval [CI]: 7.260-25.994) in infectious complications compared to those with PIV ≤ 500.2, making PIV the strongest predictor. The most significant factors in differentiating between the groups were, in order of importance, Charlson comorbidity index, stone volume, preoperative serum creatinine level, and preoperative double-J stent placement. These factors were analyzed using multivariate logistic regression alongside PIV and SII, and two models were constructed. The predictive power of Model 1 was determined as Cox & Snell R² = 0.269 and Nagelkerke R² = 0.661, while Model 2 had a Cox & Snell R² value of 0.264 and a Nagelkerke R² value of 0.648.</p><p><strong>Conclusion: </strong>PIV and SII, derived from hemogram parameters, serve as predictive inflammatory indices for postoperative infectious complications. They provide valuable preoperative insight into the patient's immune and systemic inflammatory responses. When combined with other risk factors, these indices allow for the prediction of postoperative infectious complications.</p>\",\"PeriodicalId\":9285,\"journal\":{\"name\":\"BMC Urology\",\"volume\":\"25 1\",\"pages\":\"168\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-07-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12257762/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Urology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12894-025-01859-8\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Urology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12894-025-01859-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
The role of Pan-Immune inflammation value and systemic Immune-Inflammation index as potential biomarkers in predicting infectious complications following retrograde intrarenal surgery.
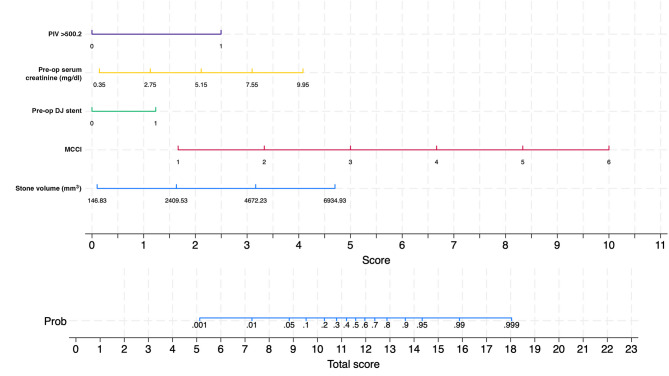
Background: To predict postoperative infectious complications by utilizing hemogram parameters and derived inflammation indices and to analyze patient-related risk factors to propose a nomogram.
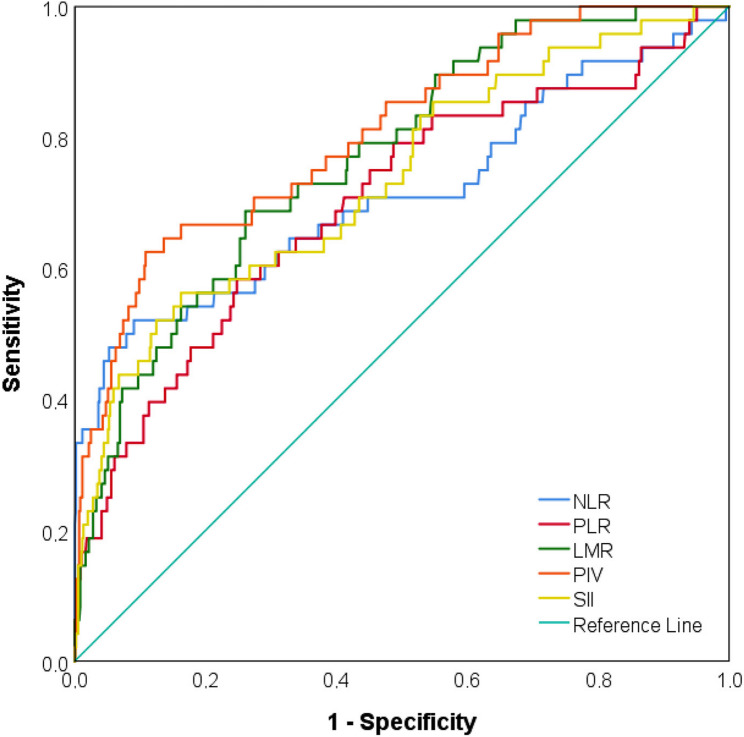
Methods: The data of patients who underwent retrograde intrarenal surgery were reviewed. The patients were categorized into two groups: those without infectious complications (Group A) and those with infectious complications (Group B). Infectious complications were defined as fever persisting above 38 °C for 48 h and the presence of two or more systemic inflammatory response syndrome (SIRS) criteria. Hemogram parameters and inflammation indices were examined to predict infectious complications. The study utilized neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR), along with the pan-immune-inflammation value (PIV) and systemic immune-inflammation index (SII).
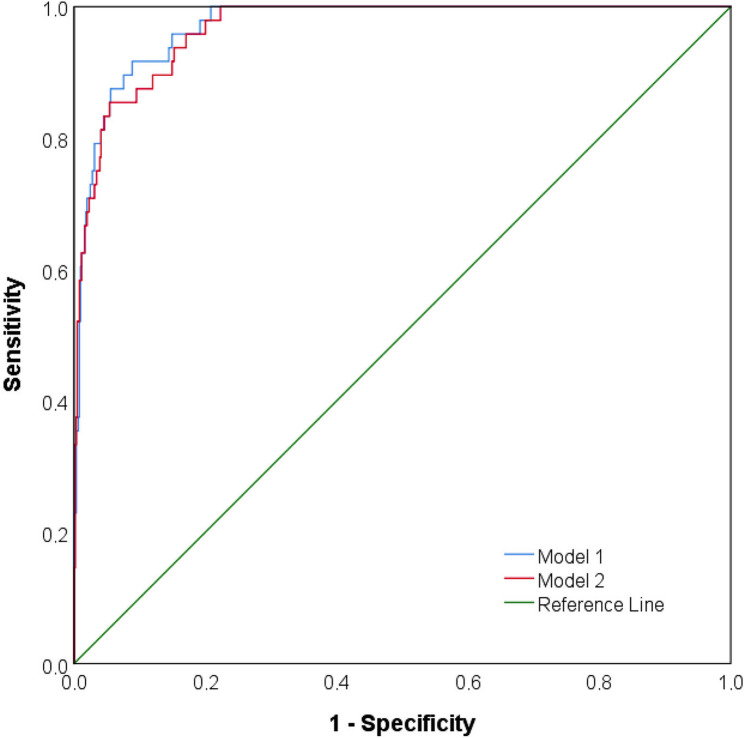
Results: The data of 658 cases were evaluated. No infectious complications were observed in 610 cases (92.7%), while 33 cases (5.0%) developed fever, and 15 cases (2.3%) met the criteria for SIRS. The optimal cut-off values for distinguishing between groups were determined as follows: >2.66 for NLR, > 122.5 for PLR, < 2.81 for LMR, > 619.4 for SII, and > 500.2 for PIV. Patients with PIV > 500.2 exhibited a 13.737-fold increase (95% confidence interval [CI]: 7.260-25.994) in infectious complications compared to those with PIV ≤ 500.2, making PIV the strongest predictor. The most significant factors in differentiating between the groups were, in order of importance, Charlson comorbidity index, stone volume, preoperative serum creatinine level, and preoperative double-J stent placement. These factors were analyzed using multivariate logistic regression alongside PIV and SII, and two models were constructed. The predictive power of Model 1 was determined as Cox & Snell R² = 0.269 and Nagelkerke R² = 0.661, while Model 2 had a Cox & Snell R² value of 0.264 and a Nagelkerke R² value of 0.648.
Conclusion: PIV and SII, derived from hemogram parameters, serve as predictive inflammatory indices for postoperative infectious complications. They provide valuable preoperative insight into the patient's immune and systemic inflammatory responses. When combined with other risk factors, these indices allow for the prediction of postoperative infectious complications.
期刊介绍:
BMC Urology is an open access journal publishing original peer-reviewed research articles in all aspects of the prevention, diagnosis and management of urological disorders, as well as related molecular genetics, pathophysiology, and epidemiology.
The journal considers manuscripts in the following broad subject-specific sections of urology:
Endourology and technology
Epidemiology and health outcomes
Pediatric urology
Pre-clinical and basic research
Reconstructive urology
Sexual function and fertility
Urological imaging
Urological oncology
Voiding dysfunction
Case reports.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


