Ben Knox-Brown, James Potts, Frits M E Franssen, Rune Nielsen, Meriam Denguezli, Anders Ørskov Rotevatn, Sanjay K Juvekar, Hamid Hacene Cherkaski, Michael Studnicka, Karl Peter Sylvester, Kevin Mortimer, Eric D Bateman, Christer Janson, Andrei Malinovschi, Terence Seemungal, Parvaiz Koul, David Mannino, Padukudru Anand Mahesh, Rain Jogi, Filip Mejza, Mohammed Al Ghobain, Stefanni Nonna M Paraguas, Tobias Welte, Emiel Wouters, Thorarinn Gislason, Imed Harrabi, Hermínia Dias, Daniel O Obaseki, Ali Kocabas, Cristina Barbara, Joao Cardoso, Dhiraj Agarwal, Asaad Ahmed Nafees, Fatima Rodrigues, Vanessa Garcia-Larsen, Gregory E Erhabor, Li-Cher Loh, Andre F S Amaral
{"title":"FVC和FEV6在阻塞性肺疾病负担(BOLD)研究中识别慢性气流阻塞和肺活量限制的一致性","authors":"Ben Knox-Brown, James Potts, Frits M E Franssen, Rune Nielsen, Meriam Denguezli, Anders Ørskov Rotevatn, Sanjay K Juvekar, Hamid Hacene Cherkaski, Michael Studnicka, Karl Peter Sylvester, Kevin Mortimer, Eric D Bateman, Christer Janson, Andrei Malinovschi, Terence Seemungal, Parvaiz Koul, David Mannino, Padukudru Anand Mahesh, Rain Jogi, Filip Mejza, Mohammed Al Ghobain, Stefanni Nonna M Paraguas, Tobias Welte, Emiel Wouters, Thorarinn Gislason, Imed Harrabi, Hermínia Dias, Daniel O Obaseki, Ali Kocabas, Cristina Barbara, Joao Cardoso, Dhiraj Agarwal, Asaad Ahmed Nafees, Fatima Rodrigues, Vanessa Garcia-Larsen, Gregory E Erhabor, Li-Cher Loh, Andre F S Amaral","doi":"10.1136/bmjresp-2024-002355","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>We investigated whether the forced expiratory volume in 6 s (FEV<sub>6</sub>) can be used as a surrogate for the forced vital capacity (FVC).</p><p><strong>Methods: </strong>The Burden of Obstructive Lung Disease is a multinational cohort study. At baseline, data were collected from adults, aged 40 years or older, from 41 sites across 34 countries. Participants from 18 sites were followed-up after a median of 8.3 years. Participants who completed the study core questionnaire and had acceptable post-bronchodilator spirometry were included. We performed receiver operating characteristic analyses to measure the ability of FEV<sub>1</sub>/FEV<sub>6</sub> less than the lower limit of normal (LLN) to correctly classify FEV<sub>1</sub>/FVC less than the LLN, and FEV<sub>6</sub> less than the LLN to correctly classify FVC less than the LLN. We used multilevel regression analyses to assess the association of discordant measurements with respiratory symptoms, quality of life and lung function decline.</p><p><strong>Results: </strong>At baseline, 28 604 participants were included. 53% were female (15 060). 10% (2876) had chronic airflow obstruction for FEV<sub>1</sub>/FVC, compared with 9% (2704) for FEV<sub>1</sub>/FEV<sub>6</sub>. 37% (10 637) had spirometric restriction for FVC, compared with 35% (9978) for FEV<sub>6</sub>. The FEV<sub>1</sub>/FEV<sub>6</sub> had excellent accuracy in identifying FEV<sub>1</sub>/FVC less than the LLN (area under the curve (AUC): 0.90, 95% CI, 0.89 to 0.91, κ coefficient 0.82). The FEV<sub>6</sub> also had excellent agreement in identifying FVC less than the LLN (AUC: 0.95, 95% CI, 0.94 to 0.95, κ coefficient 0.90). Discordant reductions in FEV<sub>1</sub>/FEV<sub>6</sub> (1%, 345) and FEV<sub>6</sub> (1%, 309) were associated with greater odds of having respiratory symptoms and a lower physical quality of life. 3870 participants were followed up. Those with discordant reductions in FEV<sub>1</sub>/FEV<sub>6</sub> and FEV<sub>6</sub> were more likely to have chronic airflow obstruction and spirometric restriction at follow-up.</p><p><strong>Conclusions: </strong>There is strong agreement between the FVC and FEV<sub>6</sub> in the identification of chronic airflow obstruction and spirometric restriction.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-07-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12258291/pdf/","citationCount":"0","resultStr":"{\"title\":\"Concordance between FVC and FEV<sub>6</sub> for identifying chronic airflow obstruction and spirometric restriction in the Burden of Obstructive Lung Disease (BOLD) study.\",\"authors\":\"Ben Knox-Brown, James Potts, Frits M E Franssen, Rune Nielsen, Meriam Denguezli, Anders Ørskov Rotevatn, Sanjay K Juvekar, Hamid Hacene Cherkaski, Michael Studnicka, Karl Peter Sylvester, Kevin Mortimer, Eric D Bateman, Christer Janson, Andrei Malinovschi, Terence Seemungal, Parvaiz Koul, David Mannino, Padukudru Anand Mahesh, Rain Jogi, Filip Mejza, Mohammed Al Ghobain, Stefanni Nonna M Paraguas, Tobias Welte, Emiel Wouters, Thorarinn Gislason, Imed Harrabi, Hermínia Dias, Daniel O Obaseki, Ali Kocabas, Cristina Barbara, Joao Cardoso, Dhiraj Agarwal, Asaad Ahmed Nafees, Fatima Rodrigues, Vanessa Garcia-Larsen, Gregory E Erhabor, Li-Cher Loh, Andre F S Amaral\",\"doi\":\"10.1136/bmjresp-2024-002355\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>We investigated whether the forced expiratory volume in 6 s (FEV<sub>6</sub>) can be used as a surrogate for the forced vital capacity (FVC).</p><p><strong>Methods: </strong>The Burden of Obstructive Lung Disease is a multinational cohort study. At baseline, data were collected from adults, aged 40 years or older, from 41 sites across 34 countries. Participants from 18 sites were followed-up after a median of 8.3 years. Participants who completed the study core questionnaire and had acceptable post-bronchodilator spirometry were included. We performed receiver operating characteristic analyses to measure the ability of FEV<sub>1</sub>/FEV<sub>6</sub> less than the lower limit of normal (LLN) to correctly classify FEV<sub>1</sub>/FVC less than the LLN, and FEV<sub>6</sub> less than the LLN to correctly classify FVC less than the LLN. We used multilevel regression analyses to assess the association of discordant measurements with respiratory symptoms, quality of life and lung function decline.</p><p><strong>Results: </strong>At baseline, 28 604 participants were included. 53% were female (15 060). 10% (2876) had chronic airflow obstruction for FEV<sub>1</sub>/FVC, compared with 9% (2704) for FEV<sub>1</sub>/FEV<sub>6</sub>. 37% (10 637) had spirometric restriction for FVC, compared with 35% (9978) for FEV<sub>6</sub>. The FEV<sub>1</sub>/FEV<sub>6</sub> had excellent accuracy in identifying FEV<sub>1</sub>/FVC less than the LLN (area under the curve (AUC): 0.90, 95% CI, 0.89 to 0.91, κ coefficient 0.82). The FEV<sub>6</sub> also had excellent agreement in identifying FVC less than the LLN (AUC: 0.95, 95% CI, 0.94 to 0.95, κ coefficient 0.90). Discordant reductions in FEV<sub>1</sub>/FEV<sub>6</sub> (1%, 345) and FEV<sub>6</sub> (1%, 309) were associated with greater odds of having respiratory symptoms and a lower physical quality of life. 3870 participants were followed up. Those with discordant reductions in FEV<sub>1</sub>/FEV<sub>6</sub> and FEV<sub>6</sub> were more likely to have chronic airflow obstruction and spirometric restriction at follow-up.</p><p><strong>Conclusions: </strong>There is strong agreement between the FVC and FEV<sub>6</sub> in the identification of chronic airflow obstruction and spirometric restriction.</p>\",\"PeriodicalId\":9048,\"journal\":{\"name\":\"BMJ Open Respiratory Research\",\"volume\":\"12 1\",\"pages\":\"\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-07-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12258291/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Respiratory Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjresp-2024-002355\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2024-002355","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Concordance between FVC and FEV6 for identifying chronic airflow obstruction and spirometric restriction in the Burden of Obstructive Lung Disease (BOLD) study.
Introduction: We investigated whether the forced expiratory volume in 6 s (FEV6) can be used as a surrogate for the forced vital capacity (FVC).
Methods: The Burden of Obstructive Lung Disease is a multinational cohort study. At baseline, data were collected from adults, aged 40 years or older, from 41 sites across 34 countries. Participants from 18 sites were followed-up after a median of 8.3 years. Participants who completed the study core questionnaire and had acceptable post-bronchodilator spirometry were included. We performed receiver operating characteristic analyses to measure the ability of FEV1/FEV6 less than the lower limit of normal (LLN) to correctly classify FEV1/FVC less than the LLN, and FEV6 less than the LLN to correctly classify FVC less than the LLN. We used multilevel regression analyses to assess the association of discordant measurements with respiratory symptoms, quality of life and lung function decline.
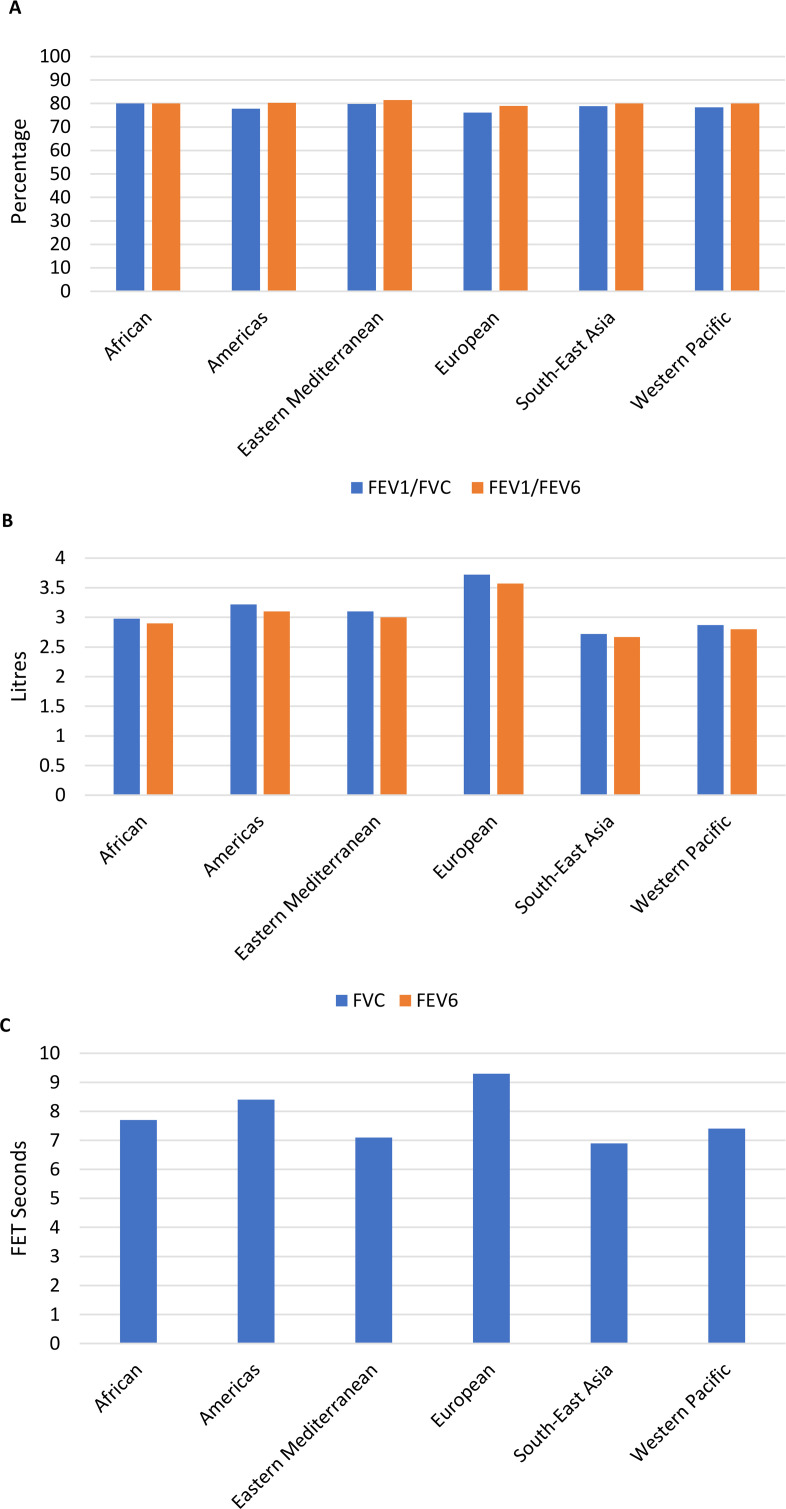
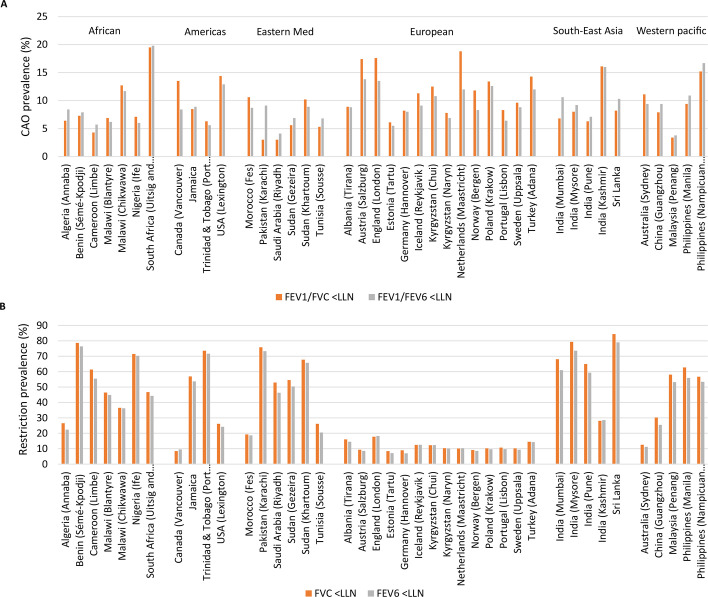
Results: At baseline, 28 604 participants were included. 53% were female (15 060). 10% (2876) had chronic airflow obstruction for FEV1/FVC, compared with 9% (2704) for FEV1/FEV6. 37% (10 637) had spirometric restriction for FVC, compared with 35% (9978) for FEV6. The FEV1/FEV6 had excellent accuracy in identifying FEV1/FVC less than the LLN (area under the curve (AUC): 0.90, 95% CI, 0.89 to 0.91, κ coefficient 0.82). The FEV6 also had excellent agreement in identifying FVC less than the LLN (AUC: 0.95, 95% CI, 0.94 to 0.95, κ coefficient 0.90). Discordant reductions in FEV1/FEV6 (1%, 345) and FEV6 (1%, 309) were associated with greater odds of having respiratory symptoms and a lower physical quality of life. 3870 participants were followed up. Those with discordant reductions in FEV1/FEV6 and FEV6 were more likely to have chronic airflow obstruction and spirometric restriction at follow-up.
Conclusions: There is strong agreement between the FVC and FEV6 in the identification of chronic airflow obstruction and spirometric restriction.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


