Sarah Dingli, Paul Rothweiler, Moritz Binder, Joselle Cook, Morie A. Gertz, Suzanne Hayman, Prashant Kapoor, Taxiarchis Kourelis, Shaji K. Kumar, Mustaqeem Siddiqui, Rahma Warsame, Yi Lin, Arthur G. Erdman, David Dingli
{"title":"嵌合抗原受体T细胞治疗不合规格产品多发性骨髓瘤的淋巴细胞动力学和结果","authors":"Sarah Dingli, Paul Rothweiler, Moritz Binder, Joselle Cook, Morie A. Gertz, Suzanne Hayman, Prashant Kapoor, Taxiarchis Kourelis, Shaji K. Kumar, Mustaqeem Siddiqui, Rahma Warsame, Yi Lin, Arthur G. Erdman, David Dingli","doi":"10.1002/ajh.70001","DOIUrl":null,"url":null,"abstract":"<p>The treatment of multiple myeloma has changed dramatically over the last two decades, fueled by a better understanding of disease biology and the identification of novel targets that led to the development of highly active therapeutics including monoclonal antibodies, bispecific antibodies and chimeric antigen receptor T cells (CAR-T) [<span>1-6</span>]. Except for CAR-T cells, all other therapeutics are manufactured and ready for use when the patient needs them. In contrast, the current state of CAR-T cells requires leukapheresis of the patient's own lymphocytes for manufacturing of a personalized product over the course of several weeks. Although the process for manufacturing is standardized and highly regulated, the state of the cells collected for manufacturing may vary and this can lead to the production of CAR-T cells that do not meet specification criteria as required by the Food and Drug Administration (FDA). The reasons for these out of specification (OOS) products may vary. However, often the patient and physician are compelled to proceed with the use of the product since therapeutic options may be limited. Therefore, it is important to determine whether the use of these OOS products is associated with any difference in outcomes, even though the data from the clinical trials that led to the approval of both idecabtagene vicleucel (Ide-cel, brand name Abecma) and ciltacabtagene autoleucel (Cilta-cel, brand name Carvykti) showed that patients may experience responses at doses considered to be “suboptimal” and below the thresholds required by the FDA [<span>1-3</span>]. We have compared the outcomes of patients who received products that were both according to specifications as well as OOS at our institution. The kinetics of lymphocyte recovery and various metrics that have been shown to impact response and durability are reported.</p><p>In the interval between June 2021 and September 2024, 134 patients have been treated with commercially approved CAR-T for multiple myeloma after their FDA approval. Only two patients treated with Ide-cel had an OOS product infused and therefore, this analysis is restricted to patients treated with Cilta-cel. We identified 22 (30.1%) patients who received OOS ciltacabtagene and 51 patients who received the in-spec product. The baseline demographic, clinical, and laboratory characteristics of these patients are summarized in Table S1. There were no significant differences in the patients' demographics, age, number of lines of therapy, cytogenetically (FISH defined high-risk disease), the presence of extramedullary disease (EMD), baseline serum ferritin, or CRP obtained prior to the start of LD chemotherapy. We also found no difference in the brain to liver glucose ratio (B2LR) determined by PET/CT before the start of LD chemotherapy of patients treated with in-spec or OOS product (<i>p</i> = 0.3324). Similarly, the fraction of patients with a B2LR ≤ 2.5 was similar (<i>p</i> = 0.2631), suggesting that the disease biology of the two cohorts was similar.</p><p>The incidence of CRS was 62.8% in patients receiving in-spec product and 45.5% with the OOS product, with no difference in CRS duration between the two groups. ICANS occurred in 5.9% of patients with the in-spec product and in 18.8% with the OOS product. The duration of ICANS was shorter in patients who received the OOS product (<i>p</i> = 0.0369).</p><p>Lymphocyte kinetics post CAR-T has been shown to influence outcomes after CAR-T [<span>7-9</span>]. We compared ALC kinetics in the two cohorts of patients. As can be seen from Table 1, there were significant differences in the ALC on various days early after CAR-T, and the recovery of the ALC was slower in patients who received an OOS product. This is also reflected in the estimated rate of lymphocyte replication (<i>k</i>) and doubling time (Table 1). The peak ALC achieved (L<sub>max</sub>) was also lower in patients with the OOS product. However, by day 15 after CAR-T, there appeared to be no difference between the two cohorts. Moreover, the proportion of patients who achieved an ALC > 1 × 10<sup>9</sup>/L was similar across the two cohorts (<i>p</i> = 0.1277).</p><p>At 3 months after CAR-T, none of the patients who received in spec product had progressed, with 77.5% having a VGPR or better response. The same depth of response was seen in 66.7% of patients treated with the OOS product (<i>p</i> = 0.5359, Fisher exact test) but two patients in the latter cohort had progressed in that time interval. There was a trend for a lower frequency of MRD negativity at 1 month after CAR-T therapy in patients who received an OOS product (<i>p</i> = 0.087). However, there was no difference in the frequency of MRD negative bone marrow results at 3 months after CAR-T (<i>p</i> = 0.4327) (Table S1).</p><p>With a median follow up of 1.4 years since therapy with Cilta-cel, two patients with OOS product have progressed compared to four patients who received an in-spec product. The median PFS for patients with an in-spec product was 1.34 years, while those who received an OOS product have a median PFS of 1.77 years (<i>p</i> = 0.2166, log-rank test) (Figure 1A). With respect to OS, we found no difference between patients with in-spec versus OOS product infused with medians of 1.34 versus 1.77 years respectively (<i>p</i> = 0.1668, log-rank test) (Figure 1B).</p><p>Given the limited number of patients, we restricted our study to univariate analysis of parameters that could impact both PFS and OS. These are reported in Table S2 (for PFS) and Table S3 (for OS). The impact of Lmax on both PFS and OS was confirmed, but achieving an ALC > 1 × 10<sup>9</sup>/L was not significant either for PFS (<i>p</i> = 0.1265) or for OS (<i>p</i> = 0.1329). However, it is pertinent to note that the median Lmax was > 1 × 10<sup>9</sup>/L for both patient cohorts (Table 1).</p><p>Manufacturing of CAR-T cells for patients with relapsed and refractory multiple myeloma is influenced by many variables, including the disease state, lines of therapy, and types of therapy received [<span>6</span>] and perhaps as yet other undefined characteristics. Although in the pivotal trials leading to the approval of these products, patients had responses at various cell dose levels [<span>1-3</span>], the definition of OOS product is not restricted to the number of cells infused alone. The description also includes the number of transduced cells, CAR expression, the ability of the lymphocytes to expand in response to in vitro stimulation, viability, and function. Therefore, the manufacturing of CAR-T cells, while standardized, is sensitive to interpatient variability, leading at times to the generation of a product that does not meet FDA release criteria. However, patients and clinicians often have very little choice but to consider the use of the product regardless. As a result, it is important to evaluate the outcome of the use of such products in real-world clinical practice. In our practice, 30.1% of patients had an OOS product with Cilta-cel in the interval under study, which appears numerically higher than that reported by Sidana et al. (19%) [<span>6</span>].</p><p>Our observations provide reassurance that patients who receive an OOS product seem to have equal depth and duration of response as seen in patients who receive an in-spec product. The response rates and expected PFS and OS reported here are in line with recent real-world evidence for cilta-cel [<span>6</span>]. Our studies suggest that while early after the infusion of OOS product, ALC kinetics are slower, eventually, these cells appear to “catch up” and many patients are able to reach the critical threshold of an ALC > 1x10<sup>9</sup>/L within the first 28 days after CAR-T [<span>7-9</span>]. This factor has been shown to be an independent determinant of depth of response, PFS and OS in several studies [<span>9</span>]. Moreover, the maximum ALC count after CAR-T also correlates with outcome [<span>7, 9</span>] and in our series, <i>L</i>\n <sub>max</sub> was a major determinant of outcome. Our results suggest that while patients with in-spec products tend to have a higher <i>L</i>\n <sub>max</sub>, the median Lmax for both cohorts is well above 1.0 × 10<sup>9</sup>/L (Table 1). This explains why the Lmax is prognostic while the ALC > 1 × 10<sup>9</sup>/L loses its significance with respect to both PFS and OS. We have recently shown the tumor metabolic activity (B2LR) is an independent predictor of survival in myeloma after CAR-T therapy [<span>10</span>]. In particular, a B2LR ≤ 2.5 was associated with a very poor prognosis with respect to both PFS and OS, independent of other poor prognostic factors such as the presence of EMD. In this cohort of patients, there was no difference in the value of B2LR or the frequency of B2LR ≤ 2.5 between the two groups. We also could not find any other difference in disease biology between the two cohorts, including genetic risk, the presence of EMD, the serum ferritin, CRP or LDH before LD chemotherapy or the number of lines of therapy prior to CAR-T.</p><p>Although the number of patients in our cohort is relatively small and will require confirmation by other groups, the data so far is reassuring that patients treated with OOS cilta-cel may have equally deep and durable responses to therapy. Our cohort of patients received cilta-cel based on the then accepted standard of care, with a median of four prior lines of therapy. All patients had been exposed to immunomodulatory agents, proteasome inhibitors, and CD38 antibodies, and all patients were refractory to lenalidomide. It is possible that as CAR-T moves to earlier lines of therapy, based on the more recent FDA approvals, the frequency of OOS products could decrease. However, our observations provide reassurance that such products are effective, with no difference in depth of response or outcomes with a median of 1.5 years of follow-up after therapy.</p><p>Concept: Sarah Dingli, Paul Rothweiler, Arthur G. Erdman, and David Dingli. Data abstraction and analysis: David Dingli, manuscript preparation: Sarah Dingli and David Dingli. Critical review and final manuscript approval: Sarah Dingli, Paul Rothweiler, Arthur G. Erdman, and David Dingli. Patient care, critical review of manuscript, final approval of manuscript: Moritz Binder, Joselle Cook, Morie A. Gertz, Suzanne Hayman, Prashant Kapoor, Taxiarchis Kourelis, Shaji K. Kumar, Mustaqeem Siddiqui, Rahma Warsame, Yi Lin, David Dingli.</p><p>S.D., P.R., M.B., J.C., S.H., M.S., R.W. and A.G.E. have no disclosures. M.A.G.: Personal fees from Ionis/Akcea, honorarium from Alnylam, personal fees from Prothena, personal fees from Sanofi, personal fees from Janssen, personal fees for Data Safety Monitoring board from AbbVie & Arcellex, fees from Johnson & Johnson, honoraria from AstraZeneca, Medscape, Dava Oncology. Alexion and NCI SPORE MM SPORE 5P50 CA186781-04. P.K.: Clinical trial support with research funding to the institution from Amgen, Regeneron, Bristol Myers Squibb, Loxo Pharmaceuticals, Ichnos, Karyopharm, Sanofi, AbbVie, and GlaxoSmithKline. Honorarium from Keosys and served on the Advisory Boards of BeiGene, Mustang Bio, Janssen, Pharmacyclics, X4 Pharmaceuticals, Kite, Oncopeptides, Ascentage, Angitia Bio, GlaxoSmithKline, Sanofi, and AbbVie. T.K.: Research funding to institution: Pfizer. S.K.K.: Consulting with no personal payment: AbbVie, Amgen, ArcellX, Beigene, BMS, Carsgen, GSK, Janssen, K36, Moderna, Pfizer, Regeneron, Roche-Genentech, Sanofi, Takeda (with personal payments): CVS Caremark, BD Biosciences. Clinical trial support to institution—AbbVie, Amgen, Astra Zeneca, BMS, Carsgen, GSK, Gracell Bio, Janssen, Oricell, Roche-Genentech, Sanofi, Takeda, Telogenomics. Y.L.: Ad Boards: Janssen, Sanofi, BMS, Regeneron, Genentech, Tessera, Legend, NexT Therapeutics. Steering Committees: Janssen, Kite/Gilead. Research: Janssen, BMS. Scientific Advisory Boards: NexImmune, Caribou. Data Safety Monitoring Board: Pfizer. D.D.: Consulting with personal payment: Alexion, Apellis, Argenyx, BMS, Janssen, Regeneron, Roche-Genentech, Omeros, Sanofi, Sorrento, and Takeda. Clinical trial support to institution: K36 Therapeutics.</p><p>This study was conducted after approval from the Institutional Review Board at Mayo Clinic. All patients included in this analysis had provided written informed consent for their medical record to be used in research.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"100 9","pages":"1705-1708"},"PeriodicalIF":9.9000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.70001","citationCount":"0","resultStr":"{\"title\":\"Lymphocyte Kinetics and Outcomes of Chimeric Antigen Receptor T Cell Therapy in Multiple Myeloma With Out of Specification Products\",\"authors\":\"Sarah Dingli, Paul Rothweiler, Moritz Binder, Joselle Cook, Morie A. Gertz, Suzanne Hayman, Prashant Kapoor, Taxiarchis Kourelis, Shaji K. Kumar, Mustaqeem Siddiqui, Rahma Warsame, Yi Lin, Arthur G. Erdman, David Dingli\",\"doi\":\"10.1002/ajh.70001\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The treatment of multiple myeloma has changed dramatically over the last two decades, fueled by a better understanding of disease biology and the identification of novel targets that led to the development of highly active therapeutics including monoclonal antibodies, bispecific antibodies and chimeric antigen receptor T cells (CAR-T) [<span>1-6</span>]. Except for CAR-T cells, all other therapeutics are manufactured and ready for use when the patient needs them. In contrast, the current state of CAR-T cells requires leukapheresis of the patient's own lymphocytes for manufacturing of a personalized product over the course of several weeks. Although the process for manufacturing is standardized and highly regulated, the state of the cells collected for manufacturing may vary and this can lead to the production of CAR-T cells that do not meet specification criteria as required by the Food and Drug Administration (FDA). The reasons for these out of specification (OOS) products may vary. However, often the patient and physician are compelled to proceed with the use of the product since therapeutic options may be limited. Therefore, it is important to determine whether the use of these OOS products is associated with any difference in outcomes, even though the data from the clinical trials that led to the approval of both idecabtagene vicleucel (Ide-cel, brand name Abecma) and ciltacabtagene autoleucel (Cilta-cel, brand name Carvykti) showed that patients may experience responses at doses considered to be “suboptimal” and below the thresholds required by the FDA [<span>1-3</span>]. We have compared the outcomes of patients who received products that were both according to specifications as well as OOS at our institution. The kinetics of lymphocyte recovery and various metrics that have been shown to impact response and durability are reported.</p><p>In the interval between June 2021 and September 2024, 134 patients have been treated with commercially approved CAR-T for multiple myeloma after their FDA approval. Only two patients treated with Ide-cel had an OOS product infused and therefore, this analysis is restricted to patients treated with Cilta-cel. We identified 22 (30.1%) patients who received OOS ciltacabtagene and 51 patients who received the in-spec product. The baseline demographic, clinical, and laboratory characteristics of these patients are summarized in Table S1. There were no significant differences in the patients' demographics, age, number of lines of therapy, cytogenetically (FISH defined high-risk disease), the presence of extramedullary disease (EMD), baseline serum ferritin, or CRP obtained prior to the start of LD chemotherapy. We also found no difference in the brain to liver glucose ratio (B2LR) determined by PET/CT before the start of LD chemotherapy of patients treated with in-spec or OOS product (<i>p</i> = 0.3324). Similarly, the fraction of patients with a B2LR ≤ 2.5 was similar (<i>p</i> = 0.2631), suggesting that the disease biology of the two cohorts was similar.</p><p>The incidence of CRS was 62.8% in patients receiving in-spec product and 45.5% with the OOS product, with no difference in CRS duration between the two groups. ICANS occurred in 5.9% of patients with the in-spec product and in 18.8% with the OOS product. The duration of ICANS was shorter in patients who received the OOS product (<i>p</i> = 0.0369).</p><p>Lymphocyte kinetics post CAR-T has been shown to influence outcomes after CAR-T [<span>7-9</span>]. We compared ALC kinetics in the two cohorts of patients. As can be seen from Table 1, there were significant differences in the ALC on various days early after CAR-T, and the recovery of the ALC was slower in patients who received an OOS product. This is also reflected in the estimated rate of lymphocyte replication (<i>k</i>) and doubling time (Table 1). The peak ALC achieved (L<sub>max</sub>) was also lower in patients with the OOS product. However, by day 15 after CAR-T, there appeared to be no difference between the two cohorts. Moreover, the proportion of patients who achieved an ALC > 1 × 10<sup>9</sup>/L was similar across the two cohorts (<i>p</i> = 0.1277).</p><p>At 3 months after CAR-T, none of the patients who received in spec product had progressed, with 77.5% having a VGPR or better response. The same depth of response was seen in 66.7% of patients treated with the OOS product (<i>p</i> = 0.5359, Fisher exact test) but two patients in the latter cohort had progressed in that time interval. There was a trend for a lower frequency of MRD negativity at 1 month after CAR-T therapy in patients who received an OOS product (<i>p</i> = 0.087). However, there was no difference in the frequency of MRD negative bone marrow results at 3 months after CAR-T (<i>p</i> = 0.4327) (Table S1).</p><p>With a median follow up of 1.4 years since therapy with Cilta-cel, two patients with OOS product have progressed compared to four patients who received an in-spec product. The median PFS for patients with an in-spec product was 1.34 years, while those who received an OOS product have a median PFS of 1.77 years (<i>p</i> = 0.2166, log-rank test) (Figure 1A). With respect to OS, we found no difference between patients with in-spec versus OOS product infused with medians of 1.34 versus 1.77 years respectively (<i>p</i> = 0.1668, log-rank test) (Figure 1B).</p><p>Given the limited number of patients, we restricted our study to univariate analysis of parameters that could impact both PFS and OS. These are reported in Table S2 (for PFS) and Table S3 (for OS). The impact of Lmax on both PFS and OS was confirmed, but achieving an ALC > 1 × 10<sup>9</sup>/L was not significant either for PFS (<i>p</i> = 0.1265) or for OS (<i>p</i> = 0.1329). However, it is pertinent to note that the median Lmax was > 1 × 10<sup>9</sup>/L for both patient cohorts (Table 1).</p><p>Manufacturing of CAR-T cells for patients with relapsed and refractory multiple myeloma is influenced by many variables, including the disease state, lines of therapy, and types of therapy received [<span>6</span>] and perhaps as yet other undefined characteristics. Although in the pivotal trials leading to the approval of these products, patients had responses at various cell dose levels [<span>1-3</span>], the definition of OOS product is not restricted to the number of cells infused alone. The description also includes the number of transduced cells, CAR expression, the ability of the lymphocytes to expand in response to in vitro stimulation, viability, and function. Therefore, the manufacturing of CAR-T cells, while standardized, is sensitive to interpatient variability, leading at times to the generation of a product that does not meet FDA release criteria. However, patients and clinicians often have very little choice but to consider the use of the product regardless. As a result, it is important to evaluate the outcome of the use of such products in real-world clinical practice. In our practice, 30.1% of patients had an OOS product with Cilta-cel in the interval under study, which appears numerically higher than that reported by Sidana et al. (19%) [<span>6</span>].</p><p>Our observations provide reassurance that patients who receive an OOS product seem to have equal depth and duration of response as seen in patients who receive an in-spec product. The response rates and expected PFS and OS reported here are in line with recent real-world evidence for cilta-cel [<span>6</span>]. Our studies suggest that while early after the infusion of OOS product, ALC kinetics are slower, eventually, these cells appear to “catch up” and many patients are able to reach the critical threshold of an ALC > 1x10<sup>9</sup>/L within the first 28 days after CAR-T [<span>7-9</span>]. This factor has been shown to be an independent determinant of depth of response, PFS and OS in several studies [<span>9</span>]. Moreover, the maximum ALC count after CAR-T also correlates with outcome [<span>7, 9</span>] and in our series, <i>L</i>\\n <sub>max</sub> was a major determinant of outcome. Our results suggest that while patients with in-spec products tend to have a higher <i>L</i>\\n <sub>max</sub>, the median Lmax for both cohorts is well above 1.0 × 10<sup>9</sup>/L (Table 1). This explains why the Lmax is prognostic while the ALC > 1 × 10<sup>9</sup>/L loses its significance with respect to both PFS and OS. We have recently shown the tumor metabolic activity (B2LR) is an independent predictor of survival in myeloma after CAR-T therapy [<span>10</span>]. In particular, a B2LR ≤ 2.5 was associated with a very poor prognosis with respect to both PFS and OS, independent of other poor prognostic factors such as the presence of EMD. In this cohort of patients, there was no difference in the value of B2LR or the frequency of B2LR ≤ 2.5 between the two groups. We also could not find any other difference in disease biology between the two cohorts, including genetic risk, the presence of EMD, the serum ferritin, CRP or LDH before LD chemotherapy or the number of lines of therapy prior to CAR-T.</p><p>Although the number of patients in our cohort is relatively small and will require confirmation by other groups, the data so far is reassuring that patients treated with OOS cilta-cel may have equally deep and durable responses to therapy. Our cohort of patients received cilta-cel based on the then accepted standard of care, with a median of four prior lines of therapy. All patients had been exposed to immunomodulatory agents, proteasome inhibitors, and CD38 antibodies, and all patients were refractory to lenalidomide. It is possible that as CAR-T moves to earlier lines of therapy, based on the more recent FDA approvals, the frequency of OOS products could decrease. However, our observations provide reassurance that such products are effective, with no difference in depth of response or outcomes with a median of 1.5 years of follow-up after therapy.</p><p>Concept: Sarah Dingli, Paul Rothweiler, Arthur G. Erdman, and David Dingli. Data abstraction and analysis: David Dingli, manuscript preparation: Sarah Dingli and David Dingli. Critical review and final manuscript approval: Sarah Dingli, Paul Rothweiler, Arthur G. Erdman, and David Dingli. Patient care, critical review of manuscript, final approval of manuscript: Moritz Binder, Joselle Cook, Morie A. Gertz, Suzanne Hayman, Prashant Kapoor, Taxiarchis Kourelis, Shaji K. Kumar, Mustaqeem Siddiqui, Rahma Warsame, Yi Lin, David Dingli.</p><p>S.D., P.R., M.B., J.C., S.H., M.S., R.W. and A.G.E. have no disclosures. M.A.G.: Personal fees from Ionis/Akcea, honorarium from Alnylam, personal fees from Prothena, personal fees from Sanofi, personal fees from Janssen, personal fees for Data Safety Monitoring board from AbbVie & Arcellex, fees from Johnson & Johnson, honoraria from AstraZeneca, Medscape, Dava Oncology. Alexion and NCI SPORE MM SPORE 5P50 CA186781-04. P.K.: Clinical trial support with research funding to the institution from Amgen, Regeneron, Bristol Myers Squibb, Loxo Pharmaceuticals, Ichnos, Karyopharm, Sanofi, AbbVie, and GlaxoSmithKline. Honorarium from Keosys and served on the Advisory Boards of BeiGene, Mustang Bio, Janssen, Pharmacyclics, X4 Pharmaceuticals, Kite, Oncopeptides, Ascentage, Angitia Bio, GlaxoSmithKline, Sanofi, and AbbVie. T.K.: Research funding to institution: Pfizer. S.K.K.: Consulting with no personal payment: AbbVie, Amgen, ArcellX, Beigene, BMS, Carsgen, GSK, Janssen, K36, Moderna, Pfizer, Regeneron, Roche-Genentech, Sanofi, Takeda (with personal payments): CVS Caremark, BD Biosciences. Clinical trial support to institution—AbbVie, Amgen, Astra Zeneca, BMS, Carsgen, GSK, Gracell Bio, Janssen, Oricell, Roche-Genentech, Sanofi, Takeda, Telogenomics. Y.L.: Ad Boards: Janssen, Sanofi, BMS, Regeneron, Genentech, Tessera, Legend, NexT Therapeutics. Steering Committees: Janssen, Kite/Gilead. Research: Janssen, BMS. Scientific Advisory Boards: NexImmune, Caribou. Data Safety Monitoring Board: Pfizer. D.D.: Consulting with personal payment: Alexion, Apellis, Argenyx, BMS, Janssen, Regeneron, Roche-Genentech, Omeros, Sanofi, Sorrento, and Takeda. Clinical trial support to institution: K36 Therapeutics.</p><p>This study was conducted after approval from the Institutional Review Board at Mayo Clinic. All patients included in this analysis had provided written informed consent for their medical record to be used in research.</p><p>The authors declare no conflicts of interest.</p>\",\"PeriodicalId\":7724,\"journal\":{\"name\":\"American Journal of Hematology\",\"volume\":\"100 9\",\"pages\":\"1705-1708\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2025-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.70001\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Hematology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ajh.70001\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.70001","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Lymphocyte Kinetics and Outcomes of Chimeric Antigen Receptor T Cell Therapy in Multiple Myeloma With Out of Specification Products
The treatment of multiple myeloma has changed dramatically over the last two decades, fueled by a better understanding of disease biology and the identification of novel targets that led to the development of highly active therapeutics including monoclonal antibodies, bispecific antibodies and chimeric antigen receptor T cells (CAR-T) [1-6]. Except for CAR-T cells, all other therapeutics are manufactured and ready for use when the patient needs them. In contrast, the current state of CAR-T cells requires leukapheresis of the patient's own lymphocytes for manufacturing of a personalized product over the course of several weeks. Although the process for manufacturing is standardized and highly regulated, the state of the cells collected for manufacturing may vary and this can lead to the production of CAR-T cells that do not meet specification criteria as required by the Food and Drug Administration (FDA). The reasons for these out of specification (OOS) products may vary. However, often the patient and physician are compelled to proceed with the use of the product since therapeutic options may be limited. Therefore, it is important to determine whether the use of these OOS products is associated with any difference in outcomes, even though the data from the clinical trials that led to the approval of both idecabtagene vicleucel (Ide-cel, brand name Abecma) and ciltacabtagene autoleucel (Cilta-cel, brand name Carvykti) showed that patients may experience responses at doses considered to be “suboptimal” and below the thresholds required by the FDA [1-3]. We have compared the outcomes of patients who received products that were both according to specifications as well as OOS at our institution. The kinetics of lymphocyte recovery and various metrics that have been shown to impact response and durability are reported.
In the interval between June 2021 and September 2024, 134 patients have been treated with commercially approved CAR-T for multiple myeloma after their FDA approval. Only two patients treated with Ide-cel had an OOS product infused and therefore, this analysis is restricted to patients treated with Cilta-cel. We identified 22 (30.1%) patients who received OOS ciltacabtagene and 51 patients who received the in-spec product. The baseline demographic, clinical, and laboratory characteristics of these patients are summarized in Table S1. There were no significant differences in the patients' demographics, age, number of lines of therapy, cytogenetically (FISH defined high-risk disease), the presence of extramedullary disease (EMD), baseline serum ferritin, or CRP obtained prior to the start of LD chemotherapy. We also found no difference in the brain to liver glucose ratio (B2LR) determined by PET/CT before the start of LD chemotherapy of patients treated with in-spec or OOS product (p = 0.3324). Similarly, the fraction of patients with a B2LR ≤ 2.5 was similar (p = 0.2631), suggesting that the disease biology of the two cohorts was similar.
The incidence of CRS was 62.8% in patients receiving in-spec product and 45.5% with the OOS product, with no difference in CRS duration between the two groups. ICANS occurred in 5.9% of patients with the in-spec product and in 18.8% with the OOS product. The duration of ICANS was shorter in patients who received the OOS product (p = 0.0369).
Lymphocyte kinetics post CAR-T has been shown to influence outcomes after CAR-T [7-9]. We compared ALC kinetics in the two cohorts of patients. As can be seen from Table 1, there were significant differences in the ALC on various days early after CAR-T, and the recovery of the ALC was slower in patients who received an OOS product. This is also reflected in the estimated rate of lymphocyte replication (k) and doubling time (Table 1). The peak ALC achieved (Lmax) was also lower in patients with the OOS product. However, by day 15 after CAR-T, there appeared to be no difference between the two cohorts. Moreover, the proportion of patients who achieved an ALC > 1 × 109/L was similar across the two cohorts (p = 0.1277).
At 3 months after CAR-T, none of the patients who received in spec product had progressed, with 77.5% having a VGPR or better response. The same depth of response was seen in 66.7% of patients treated with the OOS product (p = 0.5359, Fisher exact test) but two patients in the latter cohort had progressed in that time interval. There was a trend for a lower frequency of MRD negativity at 1 month after CAR-T therapy in patients who received an OOS product (p = 0.087). However, there was no difference in the frequency of MRD negative bone marrow results at 3 months after CAR-T (p = 0.4327) (Table S1).
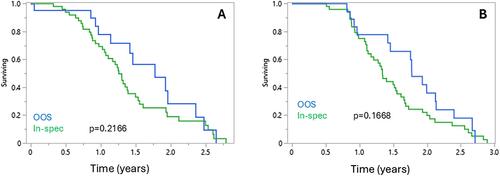
With a median follow up of 1.4 years since therapy with Cilta-cel, two patients with OOS product have progressed compared to four patients who received an in-spec product. The median PFS for patients with an in-spec product was 1.34 years, while those who received an OOS product have a median PFS of 1.77 years (p = 0.2166, log-rank test) (Figure 1A). With respect to OS, we found no difference between patients with in-spec versus OOS product infused with medians of 1.34 versus 1.77 years respectively (p = 0.1668, log-rank test) (Figure 1B).
Given the limited number of patients, we restricted our study to univariate analysis of parameters that could impact both PFS and OS. These are reported in Table S2 (for PFS) and Table S3 (for OS). The impact of Lmax on both PFS and OS was confirmed, but achieving an ALC > 1 × 109/L was not significant either for PFS (p = 0.1265) or for OS (p = 0.1329). However, it is pertinent to note that the median Lmax was > 1 × 109/L for both patient cohorts (Table 1).
Manufacturing of CAR-T cells for patients with relapsed and refractory multiple myeloma is influenced by many variables, including the disease state, lines of therapy, and types of therapy received [6] and perhaps as yet other undefined characteristics. Although in the pivotal trials leading to the approval of these products, patients had responses at various cell dose levels [1-3], the definition of OOS product is not restricted to the number of cells infused alone. The description also includes the number of transduced cells, CAR expression, the ability of the lymphocytes to expand in response to in vitro stimulation, viability, and function. Therefore, the manufacturing of CAR-T cells, while standardized, is sensitive to interpatient variability, leading at times to the generation of a product that does not meet FDA release criteria. However, patients and clinicians often have very little choice but to consider the use of the product regardless. As a result, it is important to evaluate the outcome of the use of such products in real-world clinical practice. In our practice, 30.1% of patients had an OOS product with Cilta-cel in the interval under study, which appears numerically higher than that reported by Sidana et al. (19%) [6].
Our observations provide reassurance that patients who receive an OOS product seem to have equal depth and duration of response as seen in patients who receive an in-spec product. The response rates and expected PFS and OS reported here are in line with recent real-world evidence for cilta-cel [6]. Our studies suggest that while early after the infusion of OOS product, ALC kinetics are slower, eventually, these cells appear to “catch up” and many patients are able to reach the critical threshold of an ALC > 1x109/L within the first 28 days after CAR-T [7-9]. This factor has been shown to be an independent determinant of depth of response, PFS and OS in several studies [9]. Moreover, the maximum ALC count after CAR-T also correlates with outcome [7, 9] and in our series, Lmax was a major determinant of outcome. Our results suggest that while patients with in-spec products tend to have a higher Lmax, the median Lmax for both cohorts is well above 1.0 × 109/L (Table 1). This explains why the Lmax is prognostic while the ALC > 1 × 109/L loses its significance with respect to both PFS and OS. We have recently shown the tumor metabolic activity (B2LR) is an independent predictor of survival in myeloma after CAR-T therapy [10]. In particular, a B2LR ≤ 2.5 was associated with a very poor prognosis with respect to both PFS and OS, independent of other poor prognostic factors such as the presence of EMD. In this cohort of patients, there was no difference in the value of B2LR or the frequency of B2LR ≤ 2.5 between the two groups. We also could not find any other difference in disease biology between the two cohorts, including genetic risk, the presence of EMD, the serum ferritin, CRP or LDH before LD chemotherapy or the number of lines of therapy prior to CAR-T.
Although the number of patients in our cohort is relatively small and will require confirmation by other groups, the data so far is reassuring that patients treated with OOS cilta-cel may have equally deep and durable responses to therapy. Our cohort of patients received cilta-cel based on the then accepted standard of care, with a median of four prior lines of therapy. All patients had been exposed to immunomodulatory agents, proteasome inhibitors, and CD38 antibodies, and all patients were refractory to lenalidomide. It is possible that as CAR-T moves to earlier lines of therapy, based on the more recent FDA approvals, the frequency of OOS products could decrease. However, our observations provide reassurance that such products are effective, with no difference in depth of response or outcomes with a median of 1.5 years of follow-up after therapy.
Concept: Sarah Dingli, Paul Rothweiler, Arthur G. Erdman, and David Dingli. Data abstraction and analysis: David Dingli, manuscript preparation: Sarah Dingli and David Dingli. Critical review and final manuscript approval: Sarah Dingli, Paul Rothweiler, Arthur G. Erdman, and David Dingli. Patient care, critical review of manuscript, final approval of manuscript: Moritz Binder, Joselle Cook, Morie A. Gertz, Suzanne Hayman, Prashant Kapoor, Taxiarchis Kourelis, Shaji K. Kumar, Mustaqeem Siddiqui, Rahma Warsame, Yi Lin, David Dingli.
S.D., P.R., M.B., J.C., S.H., M.S., R.W. and A.G.E. have no disclosures. M.A.G.: Personal fees from Ionis/Akcea, honorarium from Alnylam, personal fees from Prothena, personal fees from Sanofi, personal fees from Janssen, personal fees for Data Safety Monitoring board from AbbVie & Arcellex, fees from Johnson & Johnson, honoraria from AstraZeneca, Medscape, Dava Oncology. Alexion and NCI SPORE MM SPORE 5P50 CA186781-04. P.K.: Clinical trial support with research funding to the institution from Amgen, Regeneron, Bristol Myers Squibb, Loxo Pharmaceuticals, Ichnos, Karyopharm, Sanofi, AbbVie, and GlaxoSmithKline. Honorarium from Keosys and served on the Advisory Boards of BeiGene, Mustang Bio, Janssen, Pharmacyclics, X4 Pharmaceuticals, Kite, Oncopeptides, Ascentage, Angitia Bio, GlaxoSmithKline, Sanofi, and AbbVie. T.K.: Research funding to institution: Pfizer. S.K.K.: Consulting with no personal payment: AbbVie, Amgen, ArcellX, Beigene, BMS, Carsgen, GSK, Janssen, K36, Moderna, Pfizer, Regeneron, Roche-Genentech, Sanofi, Takeda (with personal payments): CVS Caremark, BD Biosciences. Clinical trial support to institution—AbbVie, Amgen, Astra Zeneca, BMS, Carsgen, GSK, Gracell Bio, Janssen, Oricell, Roche-Genentech, Sanofi, Takeda, Telogenomics. Y.L.: Ad Boards: Janssen, Sanofi, BMS, Regeneron, Genentech, Tessera, Legend, NexT Therapeutics. Steering Committees: Janssen, Kite/Gilead. Research: Janssen, BMS. Scientific Advisory Boards: NexImmune, Caribou. Data Safety Monitoring Board: Pfizer. D.D.: Consulting with personal payment: Alexion, Apellis, Argenyx, BMS, Janssen, Regeneron, Roche-Genentech, Omeros, Sanofi, Sorrento, and Takeda. Clinical trial support to institution: K36 Therapeutics.
This study was conducted after approval from the Institutional Review Board at Mayo Clinic. All patients included in this analysis had provided written informed consent for their medical record to be used in research.
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


