L C Ramsay, S K Brode, E Rea, K Barrett, A Hernandez, N Iragorri, K Liu, L Macdonald, B Sander
{"title":"对低发病率环境下结核病治疗各阶段经济成本的纵向分析。","authors":"L C Ramsay, S K Brode, E Rea, K Barrett, A Hernandez, N Iragorri, K Liu, L Macdonald, B Sander","doi":"10.5588/ijtldopen.25.0076","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Our objective was to estimate the attributable health care costs associated with TB in Ontario, Canada.</p><p><strong>Methods: </strong>We conducted an incidence-based matched cohort study among individuals diagnosed with TB between April 1, 2002 to December 31, 2016. We matched exposed individuals 1:2 to unexposed individuals using hard and propensity score matching. Using phase-of-care costing, we calculated the mean attributable costs of TB, standardized to 10-day cost, for seven phases of illness: pre-diagnosis, initial treatment, continuation phase, remainder year 1, year 2, post-TB, and prior-to-death. We estimated survival-adjusted attributable mean 1-, 2-, and 5-year costs.</p><p><strong>Results: </strong>We matched 6,456 individuals with TB to 12,443 individuals without TB. Mean (95% CI) attributable 10-day costs was highest in the pre-death phase at $2,656 ($2,207, $3,104), followed by the initial treatment phase at $1,693 ($1,608, $1,778). Hospitalization costs were the largest cost component in each phase. The mean attributable 1-, 2-, and 5-year survival-adjusted costs were $25,586, $30,178, and $33,370, respectively.</p><p><strong>Conclusion: </strong>Individuals with TB have higher health care costs over their lifetime (from pre-diagnosis until death) than individuals without TB.</p>","PeriodicalId":519984,"journal":{"name":"IJTLD open","volume":"2 7","pages":"404-411"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12248407/pdf/","citationCount":"0","resultStr":"{\"title\":\"A longitudinal analysis of the economic cost of all phases of TB care in a low incidence setting.\",\"authors\":\"L C Ramsay, S K Brode, E Rea, K Barrett, A Hernandez, N Iragorri, K Liu, L Macdonald, B Sander\",\"doi\":\"10.5588/ijtldopen.25.0076\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Our objective was to estimate the attributable health care costs associated with TB in Ontario, Canada.</p><p><strong>Methods: </strong>We conducted an incidence-based matched cohort study among individuals diagnosed with TB between April 1, 2002 to December 31, 2016. We matched exposed individuals 1:2 to unexposed individuals using hard and propensity score matching. Using phase-of-care costing, we calculated the mean attributable costs of TB, standardized to 10-day cost, for seven phases of illness: pre-diagnosis, initial treatment, continuation phase, remainder year 1, year 2, post-TB, and prior-to-death. We estimated survival-adjusted attributable mean 1-, 2-, and 5-year costs.</p><p><strong>Results: </strong>We matched 6,456 individuals with TB to 12,443 individuals without TB. Mean (95% CI) attributable 10-day costs was highest in the pre-death phase at $2,656 ($2,207, $3,104), followed by the initial treatment phase at $1,693 ($1,608, $1,778). Hospitalization costs were the largest cost component in each phase. The mean attributable 1-, 2-, and 5-year survival-adjusted costs were $25,586, $30,178, and $33,370, respectively.</p><p><strong>Conclusion: </strong>Individuals with TB have higher health care costs over their lifetime (from pre-diagnosis until death) than individuals without TB.</p>\",\"PeriodicalId\":519984,\"journal\":{\"name\":\"IJTLD open\",\"volume\":\"2 7\",\"pages\":\"404-411\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12248407/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"IJTLD open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5588/ijtldopen.25.0076\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"IJTLD open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5588/ijtldopen.25.0076","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
A longitudinal analysis of the economic cost of all phases of TB care in a low incidence setting.
Background: Our objective was to estimate the attributable health care costs associated with TB in Ontario, Canada.
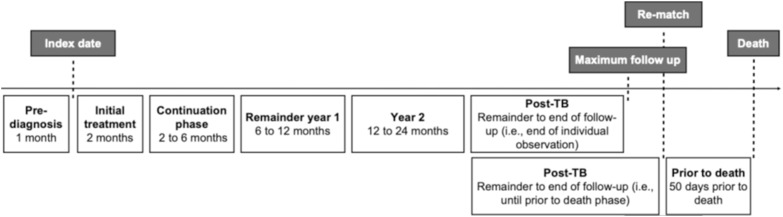
Methods: We conducted an incidence-based matched cohort study among individuals diagnosed with TB between April 1, 2002 to December 31, 2016. We matched exposed individuals 1:2 to unexposed individuals using hard and propensity score matching. Using phase-of-care costing, we calculated the mean attributable costs of TB, standardized to 10-day cost, for seven phases of illness: pre-diagnosis, initial treatment, continuation phase, remainder year 1, year 2, post-TB, and prior-to-death. We estimated survival-adjusted attributable mean 1-, 2-, and 5-year costs.
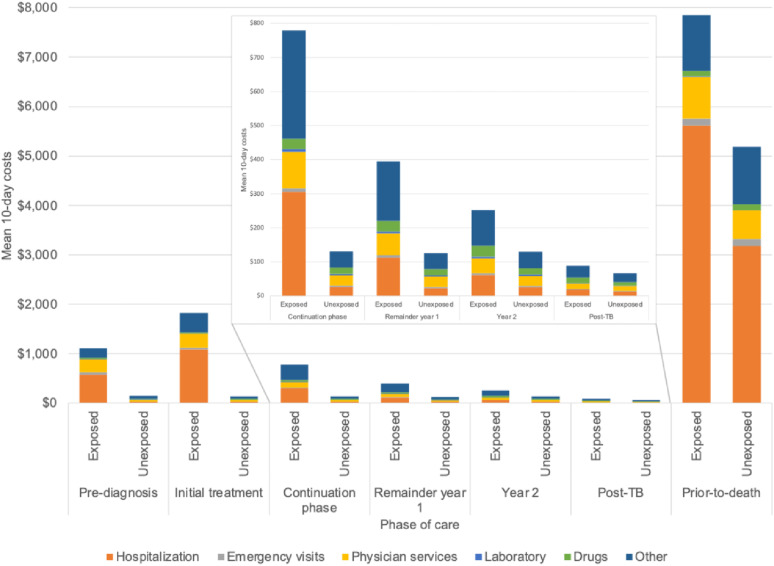
Results: We matched 6,456 individuals with TB to 12,443 individuals without TB. Mean (95% CI) attributable 10-day costs was highest in the pre-death phase at $2,656 ($2,207, $3,104), followed by the initial treatment phase at $1,693 ($1,608, $1,778). Hospitalization costs were the largest cost component in each phase. The mean attributable 1-, 2-, and 5-year survival-adjusted costs were $25,586, $30,178, and $33,370, respectively.
Conclusion: Individuals with TB have higher health care costs over their lifetime (from pre-diagnosis until death) than individuals without TB.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


