Ruben Scholten, Gerjon Hannink, Matthijs P Somford, Job L C van Susante
{"title":"反复清创、抗生素和种植体保留(DAIR)对早期假体周围关节感染的价值。","authors":"Ruben Scholten, Gerjon Hannink, Matthijs P Somford, Job L C van Susante","doi":"10.5194/jbji-10-207-2025","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background and purpose</b>: Debridement, antibiotics, and implant retention (DAIR) is the proposed initial treatment of early periprosthetic joint infection (PJI), but it may fail to provide infection control. Subsequently, either implant removal or repeated DAIR may be considered. This study aims to identify the failure rate of repeated DAIR for early PJI in primary total knee arthroplasty (TKA) and total hip arthroplasty (THA). <b>Methods:</b> All DAIRs performed following primary THA or TKA for early PJI from 2010 to 2019 were retrospectively analysed. Patient demographics, comorbidities, surgical details, and pre-DAIR C-reactive protein (CRP) levels were recorded. Failure of early infection control (within 1 month after DAIR) prompted a second DAIR. Follow-up was performed up to 2 years post-surgery. A Kaplan-Meier survival analysis was performed in single- and repeated-DAIR groups. Cox regression analyses explored potential risk factors for implant failure after repeated DAIR. <b>Results:</b> A total of 124 cases of early PJI were included. Single DAIR achieved adequate infection control in 69.4 % ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>86</mn></mrow> </math> ) of cases, while 30.6 % ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>38</mn></mrow> </math> ) of cases underwent repeated DAIR within 3-23 d. After 2 years, implant removal was performed in 8 cases (9.9 %; 95 %CI 3.0 %-16.0 %) in the single-DAIR group and in 8 cases (22.2 %; 95 %CI 7.3 %-34.7 %) in the repeated-DAIR group. No statistically significant associations between the failure of repeated DAIR and its potential risk factors were found. <b>Conclusion:</b> If initial DAIR does not achieve early PJI control, repeated DAIR can still be considered, as it may avoid implant removal in 77.8 % of cases. The authors advocate for tailored decisions considering implant revisability, patient comorbidity, and pathogen susceptibility.</p>","PeriodicalId":15271,"journal":{"name":"Journal of Bone and Joint Infection","volume":"10 4","pages":"207-215"},"PeriodicalIF":2.8000,"publicationDate":"2025-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12246790/pdf/","citationCount":"0","resultStr":"{\"title\":\"The value of repeated debridement, antibiotics, and implant retention (DAIR) for early periprosthetic joint infection.\",\"authors\":\"Ruben Scholten, Gerjon Hannink, Matthijs P Somford, Job L C van Susante\",\"doi\":\"10.5194/jbji-10-207-2025\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background and purpose</b>: Debridement, antibiotics, and implant retention (DAIR) is the proposed initial treatment of early periprosthetic joint infection (PJI), but it may fail to provide infection control. Subsequently, either implant removal or repeated DAIR may be considered. This study aims to identify the failure rate of repeated DAIR for early PJI in primary total knee arthroplasty (TKA) and total hip arthroplasty (THA). <b>Methods:</b> All DAIRs performed following primary THA or TKA for early PJI from 2010 to 2019 were retrospectively analysed. Patient demographics, comorbidities, surgical details, and pre-DAIR C-reactive protein (CRP) levels were recorded. Failure of early infection control (within 1 month after DAIR) prompted a second DAIR. Follow-up was performed up to 2 years post-surgery. A Kaplan-Meier survival analysis was performed in single- and repeated-DAIR groups. Cox regression analyses explored potential risk factors for implant failure after repeated DAIR. <b>Results:</b> A total of 124 cases of early PJI were included. Single DAIR achieved adequate infection control in 69.4 % ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>86</mn></mrow> </math> ) of cases, while 30.6 % ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>38</mn></mrow> </math> ) of cases underwent repeated DAIR within 3-23 d. After 2 years, implant removal was performed in 8 cases (9.9 %; 95 %CI 3.0 %-16.0 %) in the single-DAIR group and in 8 cases (22.2 %; 95 %CI 7.3 %-34.7 %) in the repeated-DAIR group. No statistically significant associations between the failure of repeated DAIR and its potential risk factors were found. <b>Conclusion:</b> If initial DAIR does not achieve early PJI control, repeated DAIR can still be considered, as it may avoid implant removal in 77.8 % of cases. The authors advocate for tailored decisions considering implant revisability, patient comorbidity, and pathogen susceptibility.</p>\",\"PeriodicalId\":15271,\"journal\":{\"name\":\"Journal of Bone and Joint Infection\",\"volume\":\"10 4\",\"pages\":\"207-215\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-07-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12246790/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Bone and Joint Infection\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5194/jbji-10-207-2025\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5194/jbji-10-207-2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
摘要
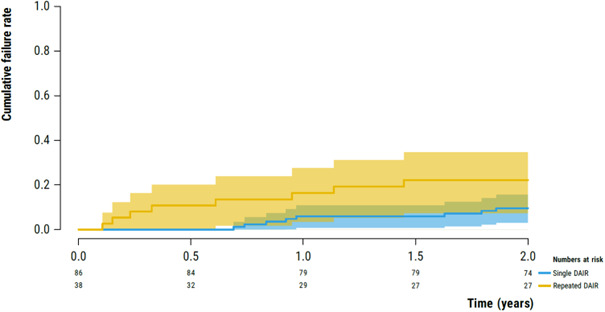
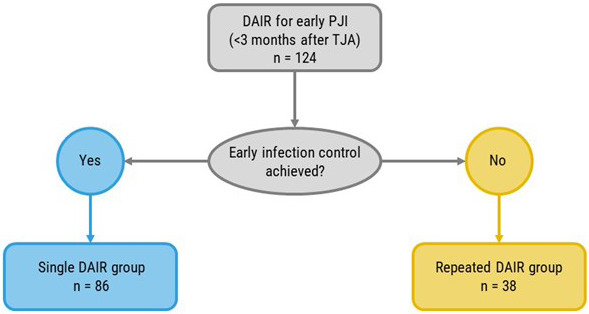
背景和目的:清创、抗生素和种植体保留(DAIR)是早期假体周围关节感染(PJI)的首选治疗方法,但它可能无法提供感染控制。随后,可以考虑取出种植体或重复DAIR。本研究旨在确定原发性全膝关节置换术(TKA)和全髋关节置换术(THA)中重复DAIR治疗早期PJI的失败率。方法:回顾性分析2010年至2019年早期PJI患者在原发性THA或TKA后进行的所有随访。记录患者人口统计、合并症、手术细节和dair前c反应蛋白(CRP)水平。早期感染控制失败(DAIR后1个月内)提示第二次DAIR。术后随访2年。对单次和重复dair组进行Kaplan-Meier生存分析。Cox回归分析探讨了重复DAIR后种植体失败的潜在危险因素。结果:共纳入124例早期PJI。69.4% (n = 86)的病例获得了良好的感染控制,而30.6% (n = 38)的病例在3-23 d内进行了多次DAIR。2年后,8例(9.9%;95% CI 3.0% - 16.0%), 8例(22.2%;95% CI 7.3% - 34.7%)。重复DAIR失败与其潜在危险因素之间无统计学意义的关联。结论:如果首次DAIR不能达到早期PJI控制,仍可考虑重复DAIR, 77.8%的病例可避免种植体拔除。作者提倡考虑植入物可修复性、患者合并症和病原体易感性的量身定制的决定。
The value of repeated debridement, antibiotics, and implant retention (DAIR) for early periprosthetic joint infection.
Background and purpose: Debridement, antibiotics, and implant retention (DAIR) is the proposed initial treatment of early periprosthetic joint infection (PJI), but it may fail to provide infection control. Subsequently, either implant removal or repeated DAIR may be considered. This study aims to identify the failure rate of repeated DAIR for early PJI in primary total knee arthroplasty (TKA) and total hip arthroplasty (THA). Methods: All DAIRs performed following primary THA or TKA for early PJI from 2010 to 2019 were retrospectively analysed. Patient demographics, comorbidities, surgical details, and pre-DAIR C-reactive protein (CRP) levels were recorded. Failure of early infection control (within 1 month after DAIR) prompted a second DAIR. Follow-up was performed up to 2 years post-surgery. A Kaplan-Meier survival analysis was performed in single- and repeated-DAIR groups. Cox regression analyses explored potential risk factors for implant failure after repeated DAIR. Results: A total of 124 cases of early PJI were included. Single DAIR achieved adequate infection control in 69.4 % ( ) of cases, while 30.6 % ( ) of cases underwent repeated DAIR within 3-23 d. After 2 years, implant removal was performed in 8 cases (9.9 %; 95 %CI 3.0 %-16.0 %) in the single-DAIR group and in 8 cases (22.2 %; 95 %CI 7.3 %-34.7 %) in the repeated-DAIR group. No statistically significant associations between the failure of repeated DAIR and its potential risk factors were found. Conclusion: If initial DAIR does not achieve early PJI control, repeated DAIR can still be considered, as it may avoid implant removal in 77.8 % of cases. The authors advocate for tailored decisions considering implant revisability, patient comorbidity, and pathogen susceptibility.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


