{"title":"日本急性胸痛患者心脏评分诊断应用的验证","authors":"Shinnosuke Nomura, Mamoru Toyofuku, Junichi Tazaki, Shojiro Tatsushima, Takanari Fujita, Shuhei Tsuji, Takahiro Iseda, Tomoya Kimura, Yuichiro Shibamori, Yuta Matsui, Kohei Ueda, Tomohiro Ichiyanagi, Akinori Yoshida, Ryo Sakamoto, Ryotaro Kai, Takeshi Morimoto, Takeshi Kimura","doi":"10.1253/circrep.CR-25-0060","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Current clinical guidelines recommend that patients with acute chest pain and suspected acute coronary syndrome (ACS) should be assessed using a risk scoring system. The History, Electrocardiogram, Age, Risk factors and Troponin (HEART) score is one such scoring system; however, large-scale validation studies remain limited in Japan.</p><p><strong>Methods and results: </strong>This study analyzed 487 patients presenting with chest pain in our emergency department (ED) between April and December 2022. We enrolled patients with suspected ACS without ST-segment elevation and shock state. The primary outcome was major adverse cardiovascular events (MACE) within 30 days following the ED visit. The endpoint occurred in 108 patients, including 90 patients with myocardial infarction. The HEART score identified 140 (28%) low-risk patients with a HEART score ≤3 who did not have any endpoint occurrence within 30 days. The area under the curve (AUC) values of the HEART score for MACE was 0.87. The results were more favorable when the highest troponin level was considered in calculating the conventional HEART score.</p><p><strong>Conclusions: </strong>The HEART score was reliable for predicting MACE within 30 days in patients presenting to the ED with chest pain in this single center study in Japan. Low-risk patients with HEART scores ≤3 can be safely ruled out for ACS. Considering the highest troponin level for scoring improved its diagnostic utility.</p>","PeriodicalId":94305,"journal":{"name":"Circulation reports","volume":"7 7","pages":"547-553"},"PeriodicalIF":1.1000,"publicationDate":"2025-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12240625/pdf/","citationCount":"0","resultStr":"{\"title\":\"Validation for the Diagnostic Use of the HEART Score in Patients With Acute Chest Pain in Japan.\",\"authors\":\"Shinnosuke Nomura, Mamoru Toyofuku, Junichi Tazaki, Shojiro Tatsushima, Takanari Fujita, Shuhei Tsuji, Takahiro Iseda, Tomoya Kimura, Yuichiro Shibamori, Yuta Matsui, Kohei Ueda, Tomohiro Ichiyanagi, Akinori Yoshida, Ryo Sakamoto, Ryotaro Kai, Takeshi Morimoto, Takeshi Kimura\",\"doi\":\"10.1253/circrep.CR-25-0060\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Current clinical guidelines recommend that patients with acute chest pain and suspected acute coronary syndrome (ACS) should be assessed using a risk scoring system. The History, Electrocardiogram, Age, Risk factors and Troponin (HEART) score is one such scoring system; however, large-scale validation studies remain limited in Japan.</p><p><strong>Methods and results: </strong>This study analyzed 487 patients presenting with chest pain in our emergency department (ED) between April and December 2022. We enrolled patients with suspected ACS without ST-segment elevation and shock state. The primary outcome was major adverse cardiovascular events (MACE) within 30 days following the ED visit. The endpoint occurred in 108 patients, including 90 patients with myocardial infarction. The HEART score identified 140 (28%) low-risk patients with a HEART score ≤3 who did not have any endpoint occurrence within 30 days. The area under the curve (AUC) values of the HEART score for MACE was 0.87. The results were more favorable when the highest troponin level was considered in calculating the conventional HEART score.</p><p><strong>Conclusions: </strong>The HEART score was reliable for predicting MACE within 30 days in patients presenting to the ED with chest pain in this single center study in Japan. Low-risk patients with HEART scores ≤3 can be safely ruled out for ACS. Considering the highest troponin level for scoring improved its diagnostic utility.</p>\",\"PeriodicalId\":94305,\"journal\":{\"name\":\"Circulation reports\",\"volume\":\"7 7\",\"pages\":\"547-553\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2025-06-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12240625/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Circulation reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1253/circrep.CR-25-0060\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/10 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-25-0060","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/10 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Validation for the Diagnostic Use of the HEART Score in Patients With Acute Chest Pain in Japan.
Background: Current clinical guidelines recommend that patients with acute chest pain and suspected acute coronary syndrome (ACS) should be assessed using a risk scoring system. The History, Electrocardiogram, Age, Risk factors and Troponin (HEART) score is one such scoring system; however, large-scale validation studies remain limited in Japan.
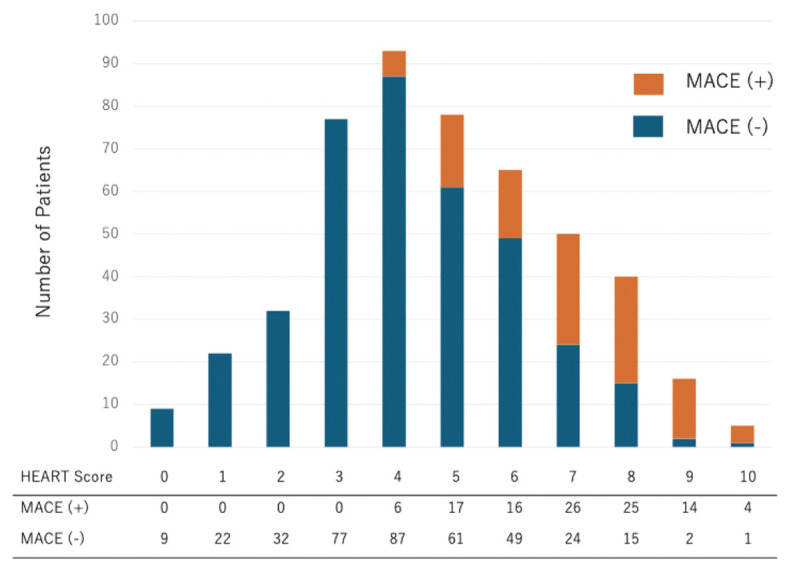
Methods and results: This study analyzed 487 patients presenting with chest pain in our emergency department (ED) between April and December 2022. We enrolled patients with suspected ACS without ST-segment elevation and shock state. The primary outcome was major adverse cardiovascular events (MACE) within 30 days following the ED visit. The endpoint occurred in 108 patients, including 90 patients with myocardial infarction. The HEART score identified 140 (28%) low-risk patients with a HEART score ≤3 who did not have any endpoint occurrence within 30 days. The area under the curve (AUC) values of the HEART score for MACE was 0.87. The results were more favorable when the highest troponin level was considered in calculating the conventional HEART score.
Conclusions: The HEART score was reliable for predicting MACE within 30 days in patients presenting to the ED with chest pain in this single center study in Japan. Low-risk patients with HEART scores ≤3 can be safely ruled out for ACS. Considering the highest troponin level for scoring improved its diagnostic utility.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


