{"title":"为瑞士肺癌患者提供基于价值的医疗保健框架——合并常规收集的医院数据的方法学方法。","authors":"Michaela Carla Barbier, Katya Galactionova, Mark Lambiris, Leonel Oliveira, Florian Rüter, Dominik Glinz, Jessica Thürmer, Flurina Pletscher, Benjamin Kasenda, Tobias Finazzi, David König, Didier Lardinois, Larissa Conrad, Leonie Mutz, Matthias Schwenkglenks","doi":"10.1371/journal.pone.0327814","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The concept of Value-Based Health Care (VBHC) seeks to maximise patient value by optimising health outcomes considering costs. However, necessary data are not readily available. In Switzerland, hospital accounting is disconnected from patient outcomes and treatment data. We demonstrate the feasibility of merging routine hospital data, including patient-reported outcome measures (PROMs), to implement core elements of VBHC in a real-world lung cancer centre.</p><p><strong>Methods: </strong>We developed a merging approach using records from 208 newly diagnosed lung cancer patients treated at University Hospital Basel between June 2020 and November 2023. Maximum patient follow-up was 12-months. Clinician-reported outcome measure (CROM) and PROM data collection followed the International Consortium for Health Outcomes Measurement (Lung Cancer Set) standard. Cost data were extracted from Switzerland's standard hospital accounting system (REKOLE®). To illustrate analytical options offered by the merged data, we analysed partial correlations between costs and utility changes from baseline.</p><p><strong>Results: </strong>The merging approach successfully allocated costs to specific lung cancer treatments and separated costs for comorbidity care, enabling an initial presentation of cost distributions for different elements of care. Median total first-year hospital costs per lung cancer patient were CHF 77,834 (mean CHF 93,621). Immunotherapy incurred the highest median costs of CHF 45,394 (mean CHF 49,518), followed by surgery of CHF 41,665 (mean CHF 48,940). First-year costs for patients diagnosed with stage I tended to be lower than for later stages. A standard graphical tool was developed to track individual patient treatment, outcome, and cost over time.</p><p><strong>Conclusions: </strong>This proof-of-concept analysis demonstrates the feasibility of a novel data merging approach as a foundation for VBHC implementation. While limited by sample size and follow-up duration, our method supports future treatment-cost-benefit models. It is reproducible and scalable across other conditions and hospitals, enabling the development of lung cancer treatments towards greater value and efficiency.</p>","PeriodicalId":20189,"journal":{"name":"PLoS ONE","volume":"20 7","pages":"e0327814"},"PeriodicalIF":2.6000,"publicationDate":"2025-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12244553/pdf/","citationCount":"0","resultStr":"{\"title\":\"Contributing to a value-based health care framework for lung cancer patients in Switzerland - A methodological approach to merge routinely collected hospital data.\",\"authors\":\"Michaela Carla Barbier, Katya Galactionova, Mark Lambiris, Leonel Oliveira, Florian Rüter, Dominik Glinz, Jessica Thürmer, Flurina Pletscher, Benjamin Kasenda, Tobias Finazzi, David König, Didier Lardinois, Larissa Conrad, Leonie Mutz, Matthias Schwenkglenks\",\"doi\":\"10.1371/journal.pone.0327814\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The concept of Value-Based Health Care (VBHC) seeks to maximise patient value by optimising health outcomes considering costs. However, necessary data are not readily available. In Switzerland, hospital accounting is disconnected from patient outcomes and treatment data. We demonstrate the feasibility of merging routine hospital data, including patient-reported outcome measures (PROMs), to implement core elements of VBHC in a real-world lung cancer centre.</p><p><strong>Methods: </strong>We developed a merging approach using records from 208 newly diagnosed lung cancer patients treated at University Hospital Basel between June 2020 and November 2023. Maximum patient follow-up was 12-months. Clinician-reported outcome measure (CROM) and PROM data collection followed the International Consortium for Health Outcomes Measurement (Lung Cancer Set) standard. Cost data were extracted from Switzerland's standard hospital accounting system (REKOLE®). To illustrate analytical options offered by the merged data, we analysed partial correlations between costs and utility changes from baseline.</p><p><strong>Results: </strong>The merging approach successfully allocated costs to specific lung cancer treatments and separated costs for comorbidity care, enabling an initial presentation of cost distributions for different elements of care. Median total first-year hospital costs per lung cancer patient were CHF 77,834 (mean CHF 93,621). Immunotherapy incurred the highest median costs of CHF 45,394 (mean CHF 49,518), followed by surgery of CHF 41,665 (mean CHF 48,940). First-year costs for patients diagnosed with stage I tended to be lower than for later stages. A standard graphical tool was developed to track individual patient treatment, outcome, and cost over time.</p><p><strong>Conclusions: </strong>This proof-of-concept analysis demonstrates the feasibility of a novel data merging approach as a foundation for VBHC implementation. While limited by sample size and follow-up duration, our method supports future treatment-cost-benefit models. It is reproducible and scalable across other conditions and hospitals, enabling the development of lung cancer treatments towards greater value and efficiency.</p>\",\"PeriodicalId\":20189,\"journal\":{\"name\":\"PLoS ONE\",\"volume\":\"20 7\",\"pages\":\"e0327814\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-07-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12244553/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS ONE\",\"FirstCategoryId\":\"103\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pone.0327814\",\"RegionNum\":3,\"RegionCategory\":\"综合性期刊\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS ONE","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1371/journal.pone.0327814","RegionNum":3,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
Contributing to a value-based health care framework for lung cancer patients in Switzerland - A methodological approach to merge routinely collected hospital data.
Background: The concept of Value-Based Health Care (VBHC) seeks to maximise patient value by optimising health outcomes considering costs. However, necessary data are not readily available. In Switzerland, hospital accounting is disconnected from patient outcomes and treatment data. We demonstrate the feasibility of merging routine hospital data, including patient-reported outcome measures (PROMs), to implement core elements of VBHC in a real-world lung cancer centre.
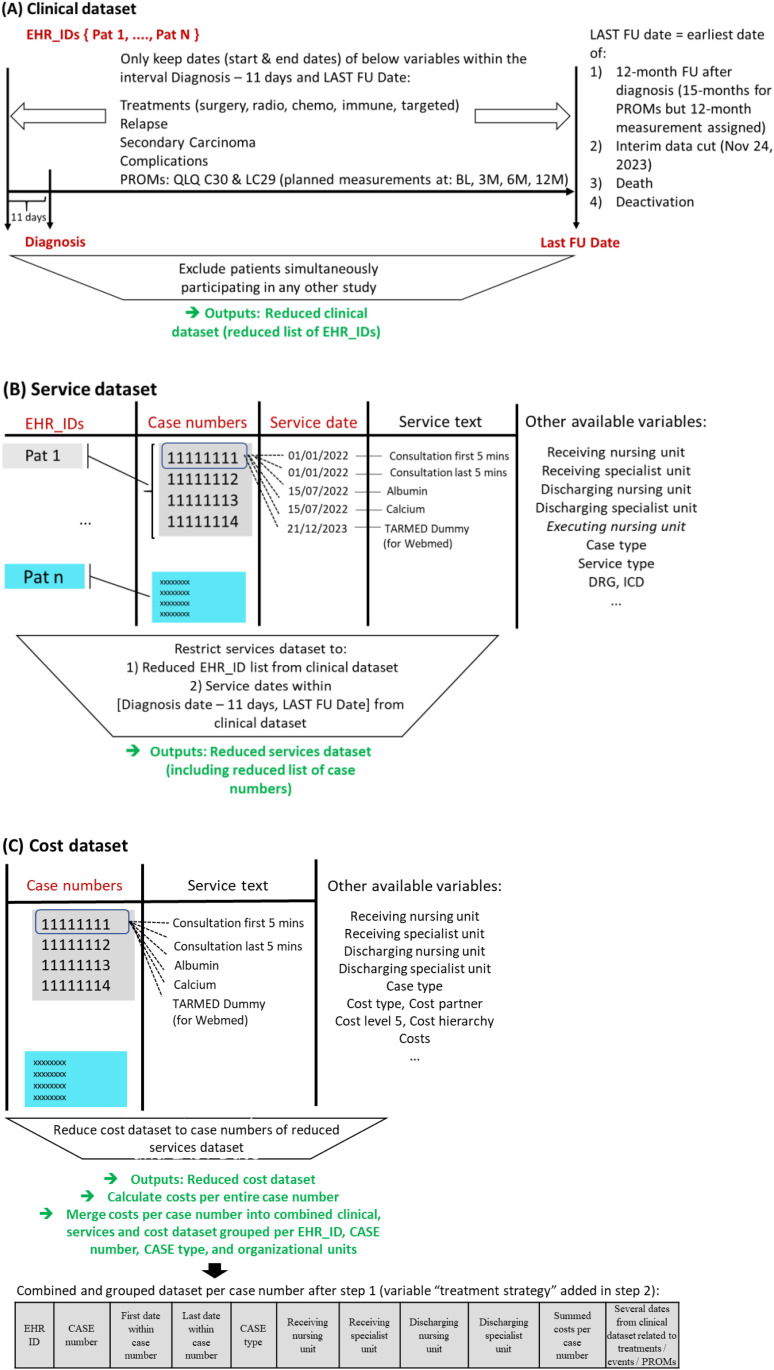
Methods: We developed a merging approach using records from 208 newly diagnosed lung cancer patients treated at University Hospital Basel between June 2020 and November 2023. Maximum patient follow-up was 12-months. Clinician-reported outcome measure (CROM) and PROM data collection followed the International Consortium for Health Outcomes Measurement (Lung Cancer Set) standard. Cost data were extracted from Switzerland's standard hospital accounting system (REKOLE®). To illustrate analytical options offered by the merged data, we analysed partial correlations between costs and utility changes from baseline.
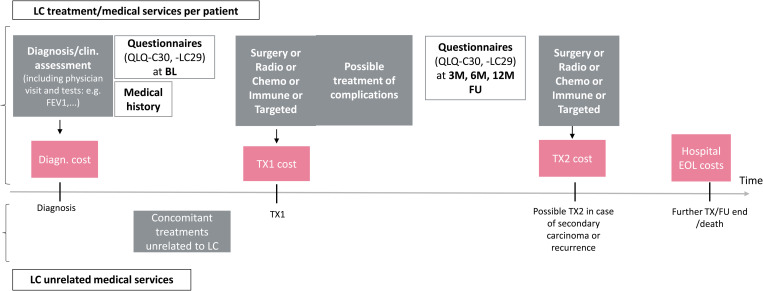
Results: The merging approach successfully allocated costs to specific lung cancer treatments and separated costs for comorbidity care, enabling an initial presentation of cost distributions for different elements of care. Median total first-year hospital costs per lung cancer patient were CHF 77,834 (mean CHF 93,621). Immunotherapy incurred the highest median costs of CHF 45,394 (mean CHF 49,518), followed by surgery of CHF 41,665 (mean CHF 48,940). First-year costs for patients diagnosed with stage I tended to be lower than for later stages. A standard graphical tool was developed to track individual patient treatment, outcome, and cost over time.
Conclusions: This proof-of-concept analysis demonstrates the feasibility of a novel data merging approach as a foundation for VBHC implementation. While limited by sample size and follow-up duration, our method supports future treatment-cost-benefit models. It is reproducible and scalable across other conditions and hospitals, enabling the development of lung cancer treatments towards greater value and efficiency.
期刊介绍:
PLOS ONE is an international, peer-reviewed, open-access, online publication. PLOS ONE welcomes reports on primary research from any scientific discipline. It provides:
* Open-access—freely accessible online, authors retain copyright
* Fast publication times
* Peer review by expert, practicing researchers
* Post-publication tools to indicate quality and impact
* Community-based dialogue on articles
* Worldwide media coverage

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


