{"title":"肠系膜上腔及门静脉血栓形成后小肠狭窄致急性肠梗阻1例。","authors":"Saurabh Raj, Rudrakshi Mahaldar, Bishal Saha, Subhra Banerjee","doi":"10.1159/000546789","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Portal vein thrombosis (PVT) is a critical factor in portal hypertension, often linked to liver disease but also occurring independently. Superior mesenteric vein thrombosis and PVT can lead to mesenteric ischemia, even without predisposing hepatic or abdominal conditions. While acute or chronic PVT may present with variable occlusion, the development of intestinal strictures is rare. Persistent symptoms necessitate close follow-up for early detection and timely intervention.</p><p><strong>Case presentation: </strong>A male patient in his early 40s presented with 15 days of progressive upper abdominal pain and one day of vomiting. He had a history of diabetes and hypertension. Examination revealed tachycardia and epigastric tenderness. Laboratory tests showed neutrophilic leukocytosis and positive occult blood in the stool. Contrast-enhanced CT (CECT) revealed PVT extending into its right branch, jejunal wall thickening, and mesenteric engorgement suggestive of ischemia. Upper GI endoscopy showed esophageal varices and portal hypertensive gastropathy. He was managed conservatively with anticoagulation and discharged. One month later, he returned with recurrent vomiting, worsened by solid food. Repeat CECT showed jejunal obstruction with a 3-cm stricture. Exploratory laparotomy revealed dense adhesions; adhesiolysis, bowel resection, anastomosis, and feeding jejunostomy were performed. Histopathological examination showed a sealed-off perforation with acute suppurative inflammation and fibrotic changes consistent with ischemic stricture.</p><p><strong>Conclusion: </strong>While mesenteric venous thrombosis is primarily managed with anticoagulation, progressive bowel strictures may develop over time, necessitating surgical intervention. Long-term follow-up is crucial, as delayed complications can arise despite initial success in preventing infarction.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"509-518"},"PeriodicalIF":0.6000,"publicationDate":"2025-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12245150/pdf/","citationCount":"0","resultStr":"{\"title\":\"Acute Intestinal Obstruction from Small Bowel Stricture following Superior Mesenteric and Portal Vein Thrombosis: A Case Report.\",\"authors\":\"Saurabh Raj, Rudrakshi Mahaldar, Bishal Saha, Subhra Banerjee\",\"doi\":\"10.1159/000546789\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Portal vein thrombosis (PVT) is a critical factor in portal hypertension, often linked to liver disease but also occurring independently. Superior mesenteric vein thrombosis and PVT can lead to mesenteric ischemia, even without predisposing hepatic or abdominal conditions. While acute or chronic PVT may present with variable occlusion, the development of intestinal strictures is rare. Persistent symptoms necessitate close follow-up for early detection and timely intervention.</p><p><strong>Case presentation: </strong>A male patient in his early 40s presented with 15 days of progressive upper abdominal pain and one day of vomiting. He had a history of diabetes and hypertension. Examination revealed tachycardia and epigastric tenderness. Laboratory tests showed neutrophilic leukocytosis and positive occult blood in the stool. Contrast-enhanced CT (CECT) revealed PVT extending into its right branch, jejunal wall thickening, and mesenteric engorgement suggestive of ischemia. Upper GI endoscopy showed esophageal varices and portal hypertensive gastropathy. He was managed conservatively with anticoagulation and discharged. One month later, he returned with recurrent vomiting, worsened by solid food. Repeat CECT showed jejunal obstruction with a 3-cm stricture. Exploratory laparotomy revealed dense adhesions; adhesiolysis, bowel resection, anastomosis, and feeding jejunostomy were performed. Histopathological examination showed a sealed-off perforation with acute suppurative inflammation and fibrotic changes consistent with ischemic stricture.</p><p><strong>Conclusion: </strong>While mesenteric venous thrombosis is primarily managed with anticoagulation, progressive bowel strictures may develop over time, necessitating surgical intervention. Long-term follow-up is crucial, as delayed complications can arise despite initial success in preventing infarction.</p>\",\"PeriodicalId\":9614,\"journal\":{\"name\":\"Case Reports in Gastroenterology\",\"volume\":\"19 1\",\"pages\":\"509-518\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2025-07-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12245150/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000546789\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000546789","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Acute Intestinal Obstruction from Small Bowel Stricture following Superior Mesenteric and Portal Vein Thrombosis: A Case Report.
Introduction: Portal vein thrombosis (PVT) is a critical factor in portal hypertension, often linked to liver disease but also occurring independently. Superior mesenteric vein thrombosis and PVT can lead to mesenteric ischemia, even without predisposing hepatic or abdominal conditions. While acute or chronic PVT may present with variable occlusion, the development of intestinal strictures is rare. Persistent symptoms necessitate close follow-up for early detection and timely intervention.
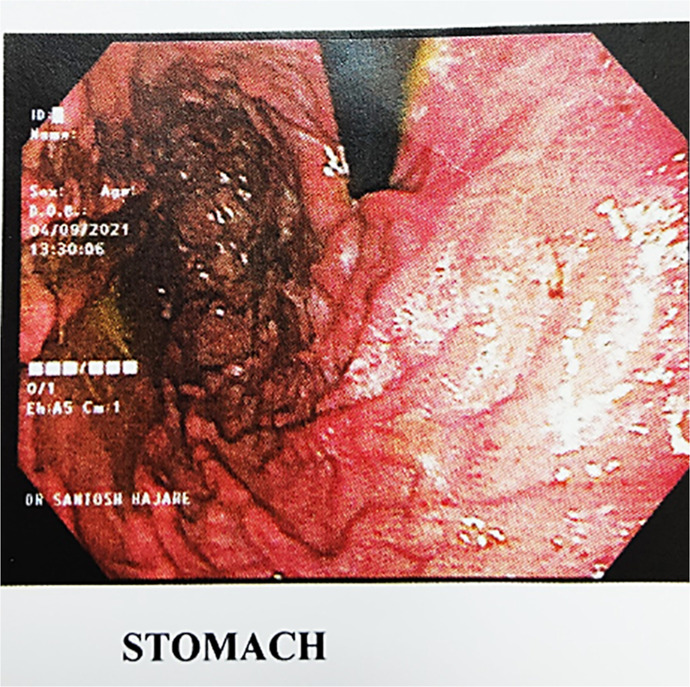
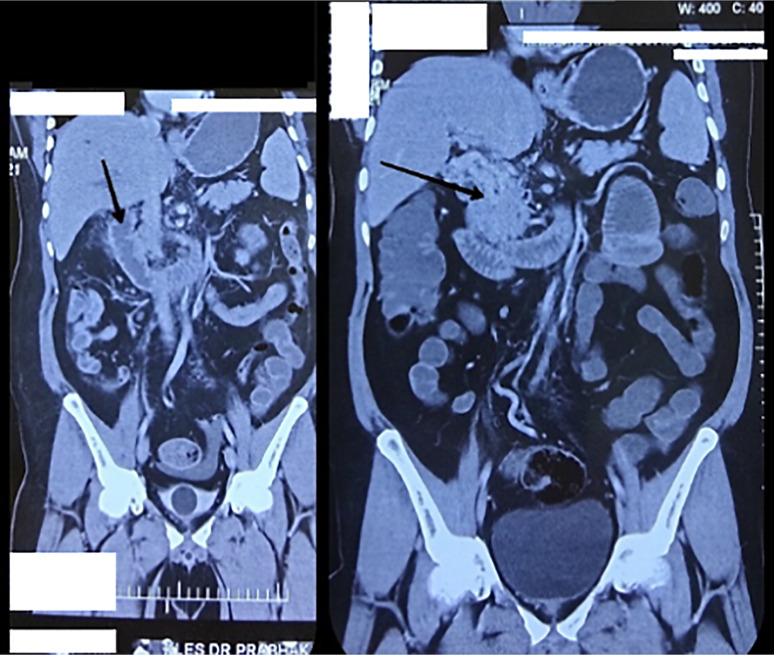
Case presentation: A male patient in his early 40s presented with 15 days of progressive upper abdominal pain and one day of vomiting. He had a history of diabetes and hypertension. Examination revealed tachycardia and epigastric tenderness. Laboratory tests showed neutrophilic leukocytosis and positive occult blood in the stool. Contrast-enhanced CT (CECT) revealed PVT extending into its right branch, jejunal wall thickening, and mesenteric engorgement suggestive of ischemia. Upper GI endoscopy showed esophageal varices and portal hypertensive gastropathy. He was managed conservatively with anticoagulation and discharged. One month later, he returned with recurrent vomiting, worsened by solid food. Repeat CECT showed jejunal obstruction with a 3-cm stricture. Exploratory laparotomy revealed dense adhesions; adhesiolysis, bowel resection, anastomosis, and feeding jejunostomy were performed. Histopathological examination showed a sealed-off perforation with acute suppurative inflammation and fibrotic changes consistent with ischemic stricture.
Conclusion: While mesenteric venous thrombosis is primarily managed with anticoagulation, progressive bowel strictures may develop over time, necessitating surgical intervention. Long-term follow-up is crucial, as delayed complications can arise despite initial success in preventing infarction.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


