John Hanna, Emily C. Zabor, Moath Albliwi, Jessica El-Asmar, Daniel P. Nurse, Ameed Bawwab, Hasan Abuamsha, Yomna Abu-Farsakh, Heya Batah, Asad Rauf, Joy Nakitandwe, David S. Bosler, Akriti G. Jain, John C. Molina, Sophia Balderman, Abhay Singh, Aaron T. Gerds, Sudipto Mukherjee, Ronald M. Sobecks, Anjali S. Advani, Hetty E. Carraway, Caroline Astbury, Moaath K. Mustafa Ali
{"title":"细胞遗传学对治疗的反应对急性髓系白血病长期生存的影响","authors":"John Hanna, Emily C. Zabor, Moath Albliwi, Jessica El-Asmar, Daniel P. Nurse, Ameed Bawwab, Hasan Abuamsha, Yomna Abu-Farsakh, Heya Batah, Asad Rauf, Joy Nakitandwe, David S. Bosler, Akriti G. Jain, John C. Molina, Sophia Balderman, Abhay Singh, Aaron T. Gerds, Sudipto Mukherjee, Ronald M. Sobecks, Anjali S. Advani, Hetty E. Carraway, Caroline Astbury, Moaath K. Mustafa Ali","doi":"10.1002/ajh.70000","DOIUrl":null,"url":null,"abstract":"<p>Prognostication in acute myeloid leukemia (AML) relies on clinical, molecular, and cytogenetic factors. In this retrospective study, we examined the impact of different levels of cytogenetic response on overall survival (OS) and event-free survival (EFS) in AML. Among 973 adult AML patients treated at Cleveland Clinic (5/2017–9/2023), 563 patients had baseline cytogenetic data and post-treatment response assessment available. Based on baseline and response cytogenetic status, patients were categorized into: normal to normal (NL-Cy to NL-Cy, <i>n</i> = 221, 39%), normal or abnormal to gain (NL/Abnl-Cy to Gain-Cy, <i>n</i> = 46, 8.2%), abnormal to persistent (Abnl-Cy to Persistent-Cy, <i>n</i> = 81, 14%), abnormal to partial response (Abnl-Cy to Partial-Cy, <i>n</i> = 20, 3.6%), and abnormal to complete response (Abnl-Cy to NL-Cy, <i>n</i> = 195, 35%). Landmark analysis was used to account for post-treatment assessments. The cohort had a median age of 62 years (interquartile range: 52–69), 256 females (45%), 90% were White, and median follow-up of 45.8 months (range: 0.73–191.3). The median OS and hazard ratios (HRs) from multivariable regression analysis were as follows: NL-Cy to NL-Cy: 37 months (95% CI: 27–91), HR = reference; NL/Abnl-Cy to Gain-Cy: 14 months (95% CI: 8.6–30), HR = 1.5 (95% CI: 0.99–2.39); Abnl-Cy to Persistent-Cy: 13 months (95% CI: 12–18), HR = 1.61 (95% CI: 1.13–2.31); Abnl-Cy to Partial-Cy: 25 months (95% CI: 14-NC), HR = 0.76 (95% CI: 0.39–1.49); and Abnl-Cy to NL-Cy: 27 months (95% CI: 19–101), HR = 1.25 (95% CI: 0.93–1.68) (<i>p</i> = 0.038). Achieving cytogenetic remission, complete or partial, was associated with better survival outcomes. These findings highlight the importance of monitoring cytogenetic responses to inform treatment decisions and support integrating cytogenetic response into risk-adapted, personalized AML management strategies.</p>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"100 9","pages":"1577-1589"},"PeriodicalIF":9.9000,"publicationDate":"2025-07-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.70000","citationCount":"0","resultStr":"{\"title\":\"Impact of Cytogenetic Response to Therapy on Long-Term Survival in Acute Myeloid Leukemia\",\"authors\":\"John Hanna, Emily C. Zabor, Moath Albliwi, Jessica El-Asmar, Daniel P. Nurse, Ameed Bawwab, Hasan Abuamsha, Yomna Abu-Farsakh, Heya Batah, Asad Rauf, Joy Nakitandwe, David S. Bosler, Akriti G. Jain, John C. Molina, Sophia Balderman, Abhay Singh, Aaron T. Gerds, Sudipto Mukherjee, Ronald M. Sobecks, Anjali S. Advani, Hetty E. Carraway, Caroline Astbury, Moaath K. Mustafa Ali\",\"doi\":\"10.1002/ajh.70000\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Prognostication in acute myeloid leukemia (AML) relies on clinical, molecular, and cytogenetic factors. In this retrospective study, we examined the impact of different levels of cytogenetic response on overall survival (OS) and event-free survival (EFS) in AML. Among 973 adult AML patients treated at Cleveland Clinic (5/2017–9/2023), 563 patients had baseline cytogenetic data and post-treatment response assessment available. Based on baseline and response cytogenetic status, patients were categorized into: normal to normal (NL-Cy to NL-Cy, <i>n</i> = 221, 39%), normal or abnormal to gain (NL/Abnl-Cy to Gain-Cy, <i>n</i> = 46, 8.2%), abnormal to persistent (Abnl-Cy to Persistent-Cy, <i>n</i> = 81, 14%), abnormal to partial response (Abnl-Cy to Partial-Cy, <i>n</i> = 20, 3.6%), and abnormal to complete response (Abnl-Cy to NL-Cy, <i>n</i> = 195, 35%). Landmark analysis was used to account for post-treatment assessments. The cohort had a median age of 62 years (interquartile range: 52–69), 256 females (45%), 90% were White, and median follow-up of 45.8 months (range: 0.73–191.3). The median OS and hazard ratios (HRs) from multivariable regression analysis were as follows: NL-Cy to NL-Cy: 37 months (95% CI: 27–91), HR = reference; NL/Abnl-Cy to Gain-Cy: 14 months (95% CI: 8.6–30), HR = 1.5 (95% CI: 0.99–2.39); Abnl-Cy to Persistent-Cy: 13 months (95% CI: 12–18), HR = 1.61 (95% CI: 1.13–2.31); Abnl-Cy to Partial-Cy: 25 months (95% CI: 14-NC), HR = 0.76 (95% CI: 0.39–1.49); and Abnl-Cy to NL-Cy: 27 months (95% CI: 19–101), HR = 1.25 (95% CI: 0.93–1.68) (<i>p</i> = 0.038). Achieving cytogenetic remission, complete or partial, was associated with better survival outcomes. These findings highlight the importance of monitoring cytogenetic responses to inform treatment decisions and support integrating cytogenetic response into risk-adapted, personalized AML management strategies.</p>\",\"PeriodicalId\":7724,\"journal\":{\"name\":\"American Journal of Hematology\",\"volume\":\"100 9\",\"pages\":\"1577-1589\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2025-07-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.70000\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Hematology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ajh.70000\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.70000","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Impact of Cytogenetic Response to Therapy on Long-Term Survival in Acute Myeloid Leukemia
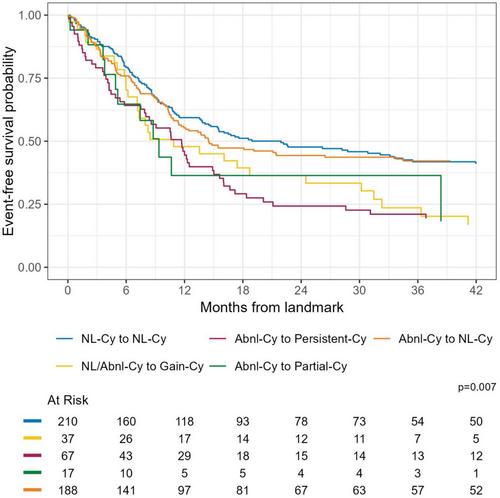
Prognostication in acute myeloid leukemia (AML) relies on clinical, molecular, and cytogenetic factors. In this retrospective study, we examined the impact of different levels of cytogenetic response on overall survival (OS) and event-free survival (EFS) in AML. Among 973 adult AML patients treated at Cleveland Clinic (5/2017–9/2023), 563 patients had baseline cytogenetic data and post-treatment response assessment available. Based on baseline and response cytogenetic status, patients were categorized into: normal to normal (NL-Cy to NL-Cy, n = 221, 39%), normal or abnormal to gain (NL/Abnl-Cy to Gain-Cy, n = 46, 8.2%), abnormal to persistent (Abnl-Cy to Persistent-Cy, n = 81, 14%), abnormal to partial response (Abnl-Cy to Partial-Cy, n = 20, 3.6%), and abnormal to complete response (Abnl-Cy to NL-Cy, n = 195, 35%). Landmark analysis was used to account for post-treatment assessments. The cohort had a median age of 62 years (interquartile range: 52–69), 256 females (45%), 90% were White, and median follow-up of 45.8 months (range: 0.73–191.3). The median OS and hazard ratios (HRs) from multivariable regression analysis were as follows: NL-Cy to NL-Cy: 37 months (95% CI: 27–91), HR = reference; NL/Abnl-Cy to Gain-Cy: 14 months (95% CI: 8.6–30), HR = 1.5 (95% CI: 0.99–2.39); Abnl-Cy to Persistent-Cy: 13 months (95% CI: 12–18), HR = 1.61 (95% CI: 1.13–2.31); Abnl-Cy to Partial-Cy: 25 months (95% CI: 14-NC), HR = 0.76 (95% CI: 0.39–1.49); and Abnl-Cy to NL-Cy: 27 months (95% CI: 19–101), HR = 1.25 (95% CI: 0.93–1.68) (p = 0.038). Achieving cytogenetic remission, complete or partial, was associated with better survival outcomes. These findings highlight the importance of monitoring cytogenetic responses to inform treatment decisions and support integrating cytogenetic response into risk-adapted, personalized AML management strategies.
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


