Aminah Sallam, Derrick Y Tam, Qiudong Chen, Allen A Razavi, Michael E Bowdish, Armin Kiankhooy, Joanna Chikwe
{"title":"二尖瓣手术时心房颤动手术消融的全国结果。","authors":"Aminah Sallam, Derrick Y Tam, Qiudong Chen, Allen A Razavi, Michael E Bowdish, Armin Kiankhooy, Joanna Chikwe","doi":"10.1093/icvts/ivaf133","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Current guidelines recommend concomitant surgical ablation at the time of mitral surgery for patients with atrial fibrillation; however, there is a paucity of data on long-term outcomes in this population. We sought to assess long-term clinical outcomes in patients undergoing concomitant surgical ablation at the time of mitral surgery.</p><p><strong>Methods: </strong>The United States Centers for Medicare and Medicaid data were used to identify patients undergoing mitral repair or replacement from 2015 to 2019. After excluding prior cardiac surgery, endocarditis and emergencies, we identified 11 410 patients undergoing isolated mitral repairs or replacement with pre-operative atrial fibrillation. Of these, 3268 (29%) received surgical ablation and 8142 (71%) did not. Propensity score matching was performed on 27 baseline characteristics. The primary outcome was freedom from death or stroke at 4 years. The secondary outcome was all-cause mortality at 4 years. Both were assessed using Cox-proportional hazard models.</p><p><strong>Results: </strong>Propensity matching yielded 3268 well-matched patient pairs (mean age: 74, 53% female, median CHA2DS2-Vasc score 4). There was no difference in all-cause mortality at 30 days (2.7% with concomitant ablation vs 2.8% without, P = 0.762). Patients undergoing concomitant ablation at the time of surgery had significantly higher freedom from death or stroke at 4 years (81% vs 77%, HR: 0.84, 95% CI 0.74-0.96). However, overall freedom from death between groups was not statistically significant (84% with concomitant ablation vs 82% without, HR: 1.14, 95% CI 0.76-1.01).</p><p><strong>Conclusions: </strong>Surgical ablation at the time of isolated mitral surgery is underutilized but associated with improved long-term outcomes.</p>","PeriodicalId":73406,"journal":{"name":"Interdisciplinary cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12258140/pdf/","citationCount":"0","resultStr":"{\"title\":\"National outcomes of surgical ablation for atrial fibrillation at the time of mitral surgery.\",\"authors\":\"Aminah Sallam, Derrick Y Tam, Qiudong Chen, Allen A Razavi, Michael E Bowdish, Armin Kiankhooy, Joanna Chikwe\",\"doi\":\"10.1093/icvts/ivaf133\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Current guidelines recommend concomitant surgical ablation at the time of mitral surgery for patients with atrial fibrillation; however, there is a paucity of data on long-term outcomes in this population. We sought to assess long-term clinical outcomes in patients undergoing concomitant surgical ablation at the time of mitral surgery.</p><p><strong>Methods: </strong>The United States Centers for Medicare and Medicaid data were used to identify patients undergoing mitral repair or replacement from 2015 to 2019. After excluding prior cardiac surgery, endocarditis and emergencies, we identified 11 410 patients undergoing isolated mitral repairs or replacement with pre-operative atrial fibrillation. Of these, 3268 (29%) received surgical ablation and 8142 (71%) did not. Propensity score matching was performed on 27 baseline characteristics. The primary outcome was freedom from death or stroke at 4 years. The secondary outcome was all-cause mortality at 4 years. Both were assessed using Cox-proportional hazard models.</p><p><strong>Results: </strong>Propensity matching yielded 3268 well-matched patient pairs (mean age: 74, 53% female, median CHA2DS2-Vasc score 4). There was no difference in all-cause mortality at 30 days (2.7% with concomitant ablation vs 2.8% without, P = 0.762). Patients undergoing concomitant ablation at the time of surgery had significantly higher freedom from death or stroke at 4 years (81% vs 77%, HR: 0.84, 95% CI 0.74-0.96). However, overall freedom from death between groups was not statistically significant (84% with concomitant ablation vs 82% without, HR: 1.14, 95% CI 0.76-1.01).</p><p><strong>Conclusions: </strong>Surgical ablation at the time of isolated mitral surgery is underutilized but associated with improved long-term outcomes.</p>\",\"PeriodicalId\":73406,\"journal\":{\"name\":\"Interdisciplinary cardiovascular and thoracic surgery\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12258140/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Interdisciplinary cardiovascular and thoracic surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/icvts/ivaf133\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"0\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interdisciplinary cardiovascular and thoracic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/icvts/ivaf133","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
目的:目前的指南建议心房颤动患者在二尖瓣手术时同时进行手术消融,但是缺乏这一人群的长期结果数据。我们试图评估在二尖瓣手术期间接受手术消融的患者的长期临床结果。方法:使用美国医疗保险和医疗补助中心的数据来识别2015年至2019年接受二尖瓣修复或置换术的患者。在排除既往心脏手术、心内膜炎和紧急情况后,我们确定了11,410例术前房颤患者接受孤立二尖瓣修复或置换术。其中,3268例(29%)接受了手术消融,8142例(71%)未接受手术消融。对27个基线特征进行倾向评分匹配。主要结果是4岁时免于死亡或中风。次要结果是4年时的全因死亡率。两者均采用cox -比例风险模型进行评估。结果:倾向匹配产生了3268对匹配良好的患者(平均年龄:74岁,53%为女性,中位CHA2DS2-Vasc评分为4)。30天的全因死亡率无差异(合并消融术2.7% vs未合并消融术2.8%,p = 0.762)。在手术时接受伴随消融的患者在4年内有更高的死亡或卒中自由度(81% vs 77%, HR: 0.84, 95% CI 0.74-0.96)。然而,两组之间的总体死亡自由无统计学意义(84%合并消融vs 82%未合并消融,相对危险度:1.14,95% CI 0.76-1.01)。结论:孤立二尖瓣手术时的外科消融未得到充分利用,但与改善的长期预后相关。
National outcomes of surgical ablation for atrial fibrillation at the time of mitral surgery.
Objectives: Current guidelines recommend concomitant surgical ablation at the time of mitral surgery for patients with atrial fibrillation; however, there is a paucity of data on long-term outcomes in this population. We sought to assess long-term clinical outcomes in patients undergoing concomitant surgical ablation at the time of mitral surgery.
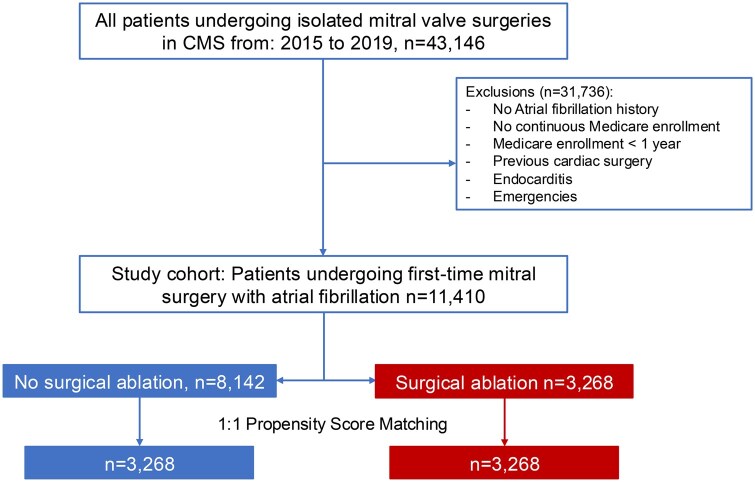
Methods: The United States Centers for Medicare and Medicaid data were used to identify patients undergoing mitral repair or replacement from 2015 to 2019. After excluding prior cardiac surgery, endocarditis and emergencies, we identified 11 410 patients undergoing isolated mitral repairs or replacement with pre-operative atrial fibrillation. Of these, 3268 (29%) received surgical ablation and 8142 (71%) did not. Propensity score matching was performed on 27 baseline characteristics. The primary outcome was freedom from death or stroke at 4 years. The secondary outcome was all-cause mortality at 4 years. Both were assessed using Cox-proportional hazard models.
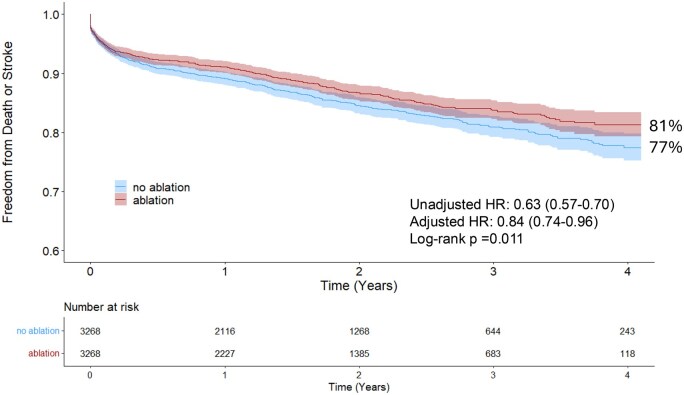
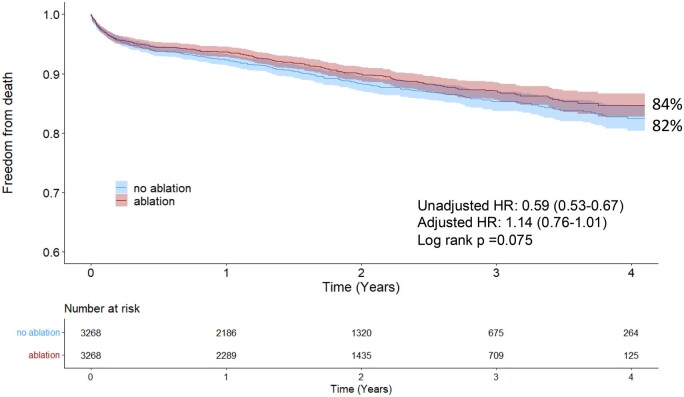
Results: Propensity matching yielded 3268 well-matched patient pairs (mean age: 74, 53% female, median CHA2DS2-Vasc score 4). There was no difference in all-cause mortality at 30 days (2.7% with concomitant ablation vs 2.8% without, P = 0.762). Patients undergoing concomitant ablation at the time of surgery had significantly higher freedom from death or stroke at 4 years (81% vs 77%, HR: 0.84, 95% CI 0.74-0.96). However, overall freedom from death between groups was not statistically significant (84% with concomitant ablation vs 82% without, HR: 1.14, 95% CI 0.76-1.01).
Conclusions: Surgical ablation at the time of isolated mitral surgery is underutilized but associated with improved long-term outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


