{"title":"优化机器人肾保留手术的ERAS方案:一项随机试验。","authors":"Yiqiang Wang, Mangmang He, Lulu Lou","doi":"10.1186/s12957-025-03927-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate the clinical efficacy of evidence-based Enhanced Recovery After Surgery (ERAS) nursing protocols in patients undergoing robotic-assisted partial nephrectomy using the Da Vinci system.</p><p><strong>Methods: </strong>A total of 240 patients undergoing Da Vinci robot-assisted partial nephrectomy were randomized (1:1) to ERAS (n = 120) or conventional care (n = 120) groups using a stratified block randomization method. The sample size was calculated based on a power of 80%, α = 0.05, and anticipated clinically significant differences, though specific values for the standard deviation and effect size were not disclosed. Primary outcomes included operative time, estimated blood loss, and length of hospital stay. Secondary outcomes assessed complication rates (Clavien-Dindo classification) and patient-reported comfort (Kolcaba GCQ questionnaire). Categorical variables were analyzed using the Chi-square test, while continuous variables were assessed with the independent samples t-test. Bonferroni correction was applied for pairwise comparisons to control for multiple testing. All analyses adhered to the modified intention-to-treat principle using the full analysis set (FAS), and no imputation was made for missing data. A p-value < 0.05 was considered statistically significant.</p><p><strong>Results: </strong>The ERAS group demonstrated superior recovery metrics compared to the control group: operative duration (228.6 ± 9.5 vs. 252.8 ± 10.1 min, mean difference [MD] - 24.2, 95% CI -27.3, -21.1; p < 0.001), intraoperative blood loss (200.4 ± 18.2 vs. 232.6 ± 19.3 mL, MD - 32.2, 95% CI -36.8, -27.6; p < 0.001), and shorter postoperative milestones (ambulation: 14.3 ± 1.7 vs. 18.7 ± 2.2 h, p < 0.001; catheter removal: 2.1 vs. 3.5 days, p < 0.001). Hospital stay was significantly reduced (6.2 ± 2.1 vs. 10.5 ± 3.3 days, MD - 4.3, 95% CI -5.0, -3.6; p < 0.001). Complication rates were markedly lower with ERAS (14.2% vs. 39.2%, relative risk [RR] 0.36, 95% CI 0.24-0.55; p < 0.001), particularly for urinary infections (3.3% vs. 11.7%, p = 0.027) and wound hematomas (5.0% vs. 13.3%, p = 0.025). GCQ scores improved significantly in the ERAS group post-intervention (p < 0.001).</p><p><strong>Conclusion: </strong>ERAS nursing grounded in evidence-based medicine significantly enhances postoperative recovery, reduces complications, and improves patient comfort in robotic-assisted partial nephrectomy. These findings support its broader clinical adoption.</p>","PeriodicalId":23856,"journal":{"name":"World Journal of Surgical Oncology","volume":"23 1","pages":"271"},"PeriodicalIF":2.5000,"publicationDate":"2025-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12243225/pdf/","citationCount":"0","resultStr":"{\"title\":\"Optimizing ERAS protocols in robotic nephron-sparing surgery: a randomized trial.\",\"authors\":\"Yiqiang Wang, Mangmang He, Lulu Lou\",\"doi\":\"10.1186/s12957-025-03927-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To evaluate the clinical efficacy of evidence-based Enhanced Recovery After Surgery (ERAS) nursing protocols in patients undergoing robotic-assisted partial nephrectomy using the Da Vinci system.</p><p><strong>Methods: </strong>A total of 240 patients undergoing Da Vinci robot-assisted partial nephrectomy were randomized (1:1) to ERAS (n = 120) or conventional care (n = 120) groups using a stratified block randomization method. The sample size was calculated based on a power of 80%, α = 0.05, and anticipated clinically significant differences, though specific values for the standard deviation and effect size were not disclosed. Primary outcomes included operative time, estimated blood loss, and length of hospital stay. Secondary outcomes assessed complication rates (Clavien-Dindo classification) and patient-reported comfort (Kolcaba GCQ questionnaire). Categorical variables were analyzed using the Chi-square test, while continuous variables were assessed with the independent samples t-test. Bonferroni correction was applied for pairwise comparisons to control for multiple testing. All analyses adhered to the modified intention-to-treat principle using the full analysis set (FAS), and no imputation was made for missing data. A p-value < 0.05 was considered statistically significant.</p><p><strong>Results: </strong>The ERAS group demonstrated superior recovery metrics compared to the control group: operative duration (228.6 ± 9.5 vs. 252.8 ± 10.1 min, mean difference [MD] - 24.2, 95% CI -27.3, -21.1; p < 0.001), intraoperative blood loss (200.4 ± 18.2 vs. 232.6 ± 19.3 mL, MD - 32.2, 95% CI -36.8, -27.6; p < 0.001), and shorter postoperative milestones (ambulation: 14.3 ± 1.7 vs. 18.7 ± 2.2 h, p < 0.001; catheter removal: 2.1 vs. 3.5 days, p < 0.001). Hospital stay was significantly reduced (6.2 ± 2.1 vs. 10.5 ± 3.3 days, MD - 4.3, 95% CI -5.0, -3.6; p < 0.001). Complication rates were markedly lower with ERAS (14.2% vs. 39.2%, relative risk [RR] 0.36, 95% CI 0.24-0.55; p < 0.001), particularly for urinary infections (3.3% vs. 11.7%, p = 0.027) and wound hematomas (5.0% vs. 13.3%, p = 0.025). GCQ scores improved significantly in the ERAS group post-intervention (p < 0.001).</p><p><strong>Conclusion: </strong>ERAS nursing grounded in evidence-based medicine significantly enhances postoperative recovery, reduces complications, and improves patient comfort in robotic-assisted partial nephrectomy. These findings support its broader clinical adoption.</p>\",\"PeriodicalId\":23856,\"journal\":{\"name\":\"World Journal of Surgical Oncology\",\"volume\":\"23 1\",\"pages\":\"271\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-07-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12243225/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Surgical Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12957-025-03927-7\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Surgical Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12957-025-03927-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Optimizing ERAS protocols in robotic nephron-sparing surgery: a randomized trial.
Objective: To evaluate the clinical efficacy of evidence-based Enhanced Recovery After Surgery (ERAS) nursing protocols in patients undergoing robotic-assisted partial nephrectomy using the Da Vinci system.
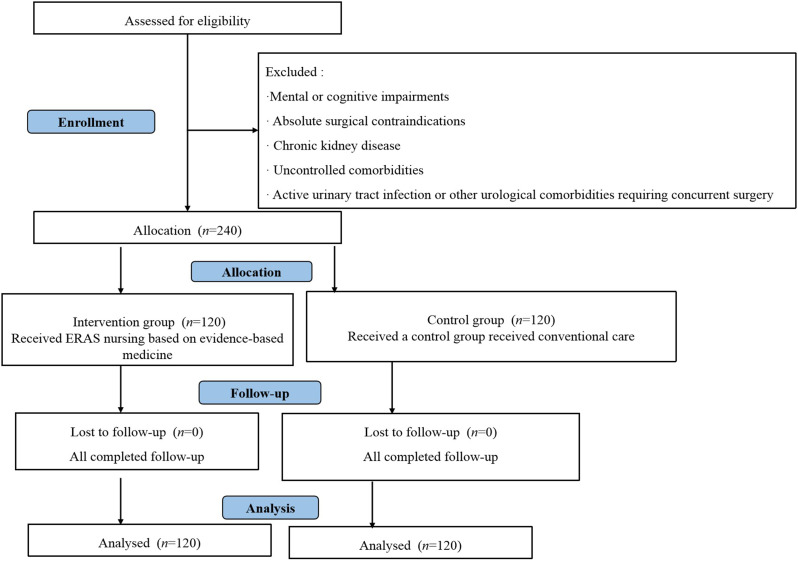
Methods: A total of 240 patients undergoing Da Vinci robot-assisted partial nephrectomy were randomized (1:1) to ERAS (n = 120) or conventional care (n = 120) groups using a stratified block randomization method. The sample size was calculated based on a power of 80%, α = 0.05, and anticipated clinically significant differences, though specific values for the standard deviation and effect size were not disclosed. Primary outcomes included operative time, estimated blood loss, and length of hospital stay. Secondary outcomes assessed complication rates (Clavien-Dindo classification) and patient-reported comfort (Kolcaba GCQ questionnaire). Categorical variables were analyzed using the Chi-square test, while continuous variables were assessed with the independent samples t-test. Bonferroni correction was applied for pairwise comparisons to control for multiple testing. All analyses adhered to the modified intention-to-treat principle using the full analysis set (FAS), and no imputation was made for missing data. A p-value < 0.05 was considered statistically significant.
Results: The ERAS group demonstrated superior recovery metrics compared to the control group: operative duration (228.6 ± 9.5 vs. 252.8 ± 10.1 min, mean difference [MD] - 24.2, 95% CI -27.3, -21.1; p < 0.001), intraoperative blood loss (200.4 ± 18.2 vs. 232.6 ± 19.3 mL, MD - 32.2, 95% CI -36.8, -27.6; p < 0.001), and shorter postoperative milestones (ambulation: 14.3 ± 1.7 vs. 18.7 ± 2.2 h, p < 0.001; catheter removal: 2.1 vs. 3.5 days, p < 0.001). Hospital stay was significantly reduced (6.2 ± 2.1 vs. 10.5 ± 3.3 days, MD - 4.3, 95% CI -5.0, -3.6; p < 0.001). Complication rates were markedly lower with ERAS (14.2% vs. 39.2%, relative risk [RR] 0.36, 95% CI 0.24-0.55; p < 0.001), particularly for urinary infections (3.3% vs. 11.7%, p = 0.027) and wound hematomas (5.0% vs. 13.3%, p = 0.025). GCQ scores improved significantly in the ERAS group post-intervention (p < 0.001).
Conclusion: ERAS nursing grounded in evidence-based medicine significantly enhances postoperative recovery, reduces complications, and improves patient comfort in robotic-assisted partial nephrectomy. These findings support its broader clinical adoption.
期刊介绍:
World Journal of Surgical Oncology publishes articles related to surgical oncology and its allied subjects, such as epidemiology, cancer research, biomarkers, prevention, pathology, radiology, cancer treatment, clinical trials, multimodality treatment and molecular biology. Emphasis is placed on original research articles. The journal also publishes significant clinical case reports, as well as balanced and timely reviews on selected topics.
Oncology is a multidisciplinary super-speciality of which surgical oncology forms an integral component, especially with solid tumors. Surgical oncologists around the world are involved in research extending from detecting the mechanisms underlying the causation of cancer, to its treatment and prevention. The role of a surgical oncologist extends across the whole continuum of care. With continued developments in diagnosis and treatment, the role of a surgical oncologist is ever-changing. Hence, World Journal of Surgical Oncology aims to keep readers abreast with latest developments that will ultimately influence the work of surgical oncologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


