Kyung Tak Oh, Avelyn Noble Lim, Alwadai Raed Ibrahim, Jang Hwan Kim
{"title":"经尿道括约肌切开术和人工尿道括约肌-一种治疗难治性膀胱排空障碍的新型两期手术:概念验证研究。","authors":"Kyung Tak Oh, Avelyn Noble Lim, Alwadai Raed Ibrahim, Jang Hwan Kim","doi":"10.5213/inj.2550016.008","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We developed an innovative 2-stage procedure combining transurethral sphincterotomy (TURS) with artificial urinary sphincter (AUS) implantation to restore voiding in patients with refractory bladder emptying disorders. This proof-of-concept study evaluated its safety and efficacy.</p><p><strong>Methods: </strong>We retrospectively reviewed clinical data from patients who underwent combined TURS and AUS implantation between April 7, 2021, and October 31, 2024. Eligible patients had neurogenic bladder with refractory emptying, irreversible neurogenic disease, and no mechanical obstruction (e.g., urethral strictures). In the TURS stage, the entire inner urethral segment corresponding to the external sphincter was resected to induce intrinsic sphincter deficiency; this was followed by AUS placement. We analyzed patient demographics, preoperative and postoperative daily pad usage, clean intermittent catheterization (CIC) frequency, patient-reported outcomes (Life Quality [LQ], International Consultation on Incontinence Questionnaire [ICIQ], Sandvik Severity Index [SAND]), postvoid residual (PVR) urine volume, estimated glomerular filtration rate (eGFR), abdominopelvic ultrasonography, and postoperative complications.</p><p><strong>Results: </strong>Four out of 6 patients (66.7%) successfully achieved CIC-free status, with effective self-voiding achieved through AUS activation and abdominal pressure generation. Significant improvements were documented in LQ scores (P=0.042), ICIQ scores (P=0.004), and SAND scores (P=0.039). Median PVR significantly decreased from 237.5 mL (interquartile range [IQR], 112.5-317.5 mL) preoperatively to 1.5 mL (IQR, 0-85.8 mL) postoperatively (P=0.028). No patient demonstrated upper-tract damage or significant eGFR change. One patient developed an AUS infection requiring explantation; another remained CIC-dependent due to insufficient abdominal pressure.</p><p><strong>Conclusion: </strong>Combining TURS with AUS implantation is a safe and effective surgical option for refractory bladder emptying disorders, yielding significant improvements in voiding autonomy and quality of life while reducing catheter dependence. Future studies with larger cohorts and longer follow-up are warranted to validate safety, long-term durability, and broader applicability. These findings may shift current paradigms in neurogenic bladder management.</p>","PeriodicalId":14466,"journal":{"name":"International Neurourology Journal","volume":"29 2","pages":"125-134"},"PeriodicalIF":2.1000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12242176/pdf/","citationCount":"0","resultStr":"{\"title\":\"Transurethral Sphincterotomy and an Artificial Urinary Sphincter - A Novel 2-Stage Surgery for Refractory Bladder Emptying Disorders: A Proof-of-Concept Study.\",\"authors\":\"Kyung Tak Oh, Avelyn Noble Lim, Alwadai Raed Ibrahim, Jang Hwan Kim\",\"doi\":\"10.5213/inj.2550016.008\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>We developed an innovative 2-stage procedure combining transurethral sphincterotomy (TURS) with artificial urinary sphincter (AUS) implantation to restore voiding in patients with refractory bladder emptying disorders. This proof-of-concept study evaluated its safety and efficacy.</p><p><strong>Methods: </strong>We retrospectively reviewed clinical data from patients who underwent combined TURS and AUS implantation between April 7, 2021, and October 31, 2024. Eligible patients had neurogenic bladder with refractory emptying, irreversible neurogenic disease, and no mechanical obstruction (e.g., urethral strictures). In the TURS stage, the entire inner urethral segment corresponding to the external sphincter was resected to induce intrinsic sphincter deficiency; this was followed by AUS placement. We analyzed patient demographics, preoperative and postoperative daily pad usage, clean intermittent catheterization (CIC) frequency, patient-reported outcomes (Life Quality [LQ], International Consultation on Incontinence Questionnaire [ICIQ], Sandvik Severity Index [SAND]), postvoid residual (PVR) urine volume, estimated glomerular filtration rate (eGFR), abdominopelvic ultrasonography, and postoperative complications.</p><p><strong>Results: </strong>Four out of 6 patients (66.7%) successfully achieved CIC-free status, with effective self-voiding achieved through AUS activation and abdominal pressure generation. Significant improvements were documented in LQ scores (P=0.042), ICIQ scores (P=0.004), and SAND scores (P=0.039). Median PVR significantly decreased from 237.5 mL (interquartile range [IQR], 112.5-317.5 mL) preoperatively to 1.5 mL (IQR, 0-85.8 mL) postoperatively (P=0.028). No patient demonstrated upper-tract damage or significant eGFR change. One patient developed an AUS infection requiring explantation; another remained CIC-dependent due to insufficient abdominal pressure.</p><p><strong>Conclusion: </strong>Combining TURS with AUS implantation is a safe and effective surgical option for refractory bladder emptying disorders, yielding significant improvements in voiding autonomy and quality of life while reducing catheter dependence. Future studies with larger cohorts and longer follow-up are warranted to validate safety, long-term durability, and broader applicability. These findings may shift current paradigms in neurogenic bladder management.</p>\",\"PeriodicalId\":14466,\"journal\":{\"name\":\"International Neurourology Journal\",\"volume\":\"29 2\",\"pages\":\"125-134\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12242176/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Neurourology Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5213/inj.2550016.008\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Neurourology Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5213/inj.2550016.008","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Transurethral Sphincterotomy and an Artificial Urinary Sphincter - A Novel 2-Stage Surgery for Refractory Bladder Emptying Disorders: A Proof-of-Concept Study.
Purpose: We developed an innovative 2-stage procedure combining transurethral sphincterotomy (TURS) with artificial urinary sphincter (AUS) implantation to restore voiding in patients with refractory bladder emptying disorders. This proof-of-concept study evaluated its safety and efficacy.
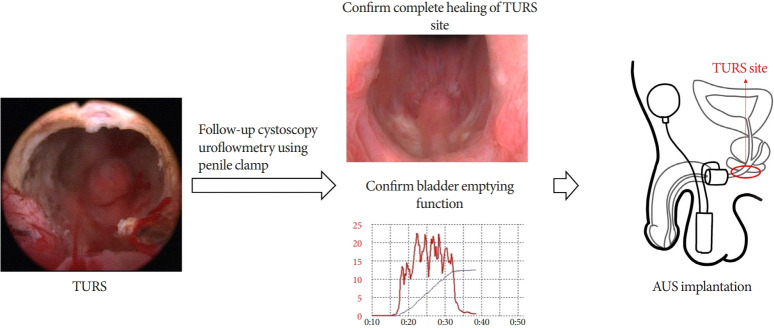
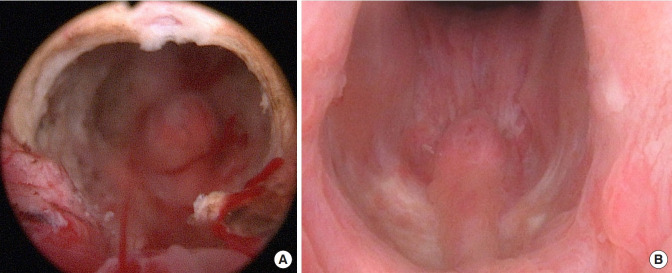
Methods: We retrospectively reviewed clinical data from patients who underwent combined TURS and AUS implantation between April 7, 2021, and October 31, 2024. Eligible patients had neurogenic bladder with refractory emptying, irreversible neurogenic disease, and no mechanical obstruction (e.g., urethral strictures). In the TURS stage, the entire inner urethral segment corresponding to the external sphincter was resected to induce intrinsic sphincter deficiency; this was followed by AUS placement. We analyzed patient demographics, preoperative and postoperative daily pad usage, clean intermittent catheterization (CIC) frequency, patient-reported outcomes (Life Quality [LQ], International Consultation on Incontinence Questionnaire [ICIQ], Sandvik Severity Index [SAND]), postvoid residual (PVR) urine volume, estimated glomerular filtration rate (eGFR), abdominopelvic ultrasonography, and postoperative complications.
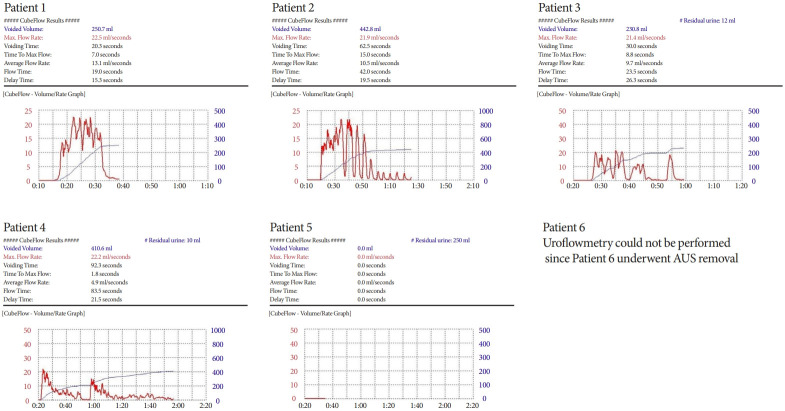
Results: Four out of 6 patients (66.7%) successfully achieved CIC-free status, with effective self-voiding achieved through AUS activation and abdominal pressure generation. Significant improvements were documented in LQ scores (P=0.042), ICIQ scores (P=0.004), and SAND scores (P=0.039). Median PVR significantly decreased from 237.5 mL (interquartile range [IQR], 112.5-317.5 mL) preoperatively to 1.5 mL (IQR, 0-85.8 mL) postoperatively (P=0.028). No patient demonstrated upper-tract damage or significant eGFR change. One patient developed an AUS infection requiring explantation; another remained CIC-dependent due to insufficient abdominal pressure.
Conclusion: Combining TURS with AUS implantation is a safe and effective surgical option for refractory bladder emptying disorders, yielding significant improvements in voiding autonomy and quality of life while reducing catheter dependence. Future studies with larger cohorts and longer follow-up are warranted to validate safety, long-term durability, and broader applicability. These findings may shift current paradigms in neurogenic bladder management.
期刊介绍:
The International Neurourology Journal (Int Neurourol J, INJ) is a quarterly international journal that publishes high-quality research papers that provide the most significant and promising achievements in the fields of clinical neurourology and fundamental science. Specifically, fundamental science includes the most influential research papers from all fields of science and technology, revolutionizing what physicians and researchers practicing the art of neurourology worldwide know. Thus, we welcome valuable basic research articles to introduce cutting-edge translational research of fundamental sciences to clinical neurourology. In the editorials, urologists will present their perspectives on these articles. The original mission statement of the INJ was published on October 12, 1997.
INJ provides authors a fast review of their work and makes a decision in an average of three to four weeks of receiving submissions. If accepted, articles are posted online in fully citable form. Supplementary issues will be published interim to quarterlies, as necessary, to fully allow berth to accept and publish relevant articles.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


