{"title":"低剂量依维莫司成功治疗一名患有结节性硬化症的学龄儿童肾血管平滑肌脂肪瘤。","authors":"Satoshi Senoo, Shoichiro Kanda, Keiichi Takizawa, Hiroshi Terashima, Yuko Kajiho, Yutaka Harita","doi":"10.1111/nep.70069","DOIUrl":null,"url":null,"abstract":"<p><p>Renal angiomyolipomas (AMLs) are a common renal manifestation in tuberous sclerosis complex (TSC), occurring in 50%-85% of cases. Even in asymptomatic individuals, treatment is often initiated based on AML size, with mTOR inhibitors being the primary medical therapy. AMLs tend to enlarge with age, and treatment during school age is rare. Secondary AML shrinkage in paediatric TSC patients has been reported who received everolimus for subependymal giant cell astrocytomas (SEGA) or epilepsy, but studies on its direct use for AMLs in paediatric cases remain limited. A 9-year-old girl born to a mother with TSC was diagnosed at birth due to cardiac rhabdomyomas, cortical tubers, and Shagreen patches. At the age of 4, ultrasound detected multiple AMLs in both kidneys, with the largest lesions measuring 2.3 cm in the right kidney and 1.6 cm in the left. By the age of 7, MRI showed further growth to 4.8 cm. Despite the absence of symptoms, the risk of haemorrhage led to treatment initiation. Everolimus was started at 1.0 mg/day (1.3 mg/m<sup>2</sup>/day), significantly lower than the standard 4.5 mg/m<sup>2</sup>/day. Trough levels remained below the target range, yet AMLs showed a shrinking tendency, with MRI at age 9 revealing a reduction in the largest AML to 2.4 cm. Stomatitis occurred intermittently, but no serious adverse effects were observed. This case suggests that low-dose everolimus can effectively reduce AML size while minimising adverse effects, highlighting its potential as a treatment option for AMLs in paediatric TSC patients.</p>","PeriodicalId":520716,"journal":{"name":"Nephrology (Carlton, Vic.)","volume":"30 7","pages":"e70069"},"PeriodicalIF":1.9000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12237548/pdf/","citationCount":"0","resultStr":"{\"title\":\"Successful Treatment of Growing Renal Angiomyolipomas With Low-Dose Everolimus in a School-Aged Child With Tuberous Sclerosis Complex.\",\"authors\":\"Satoshi Senoo, Shoichiro Kanda, Keiichi Takizawa, Hiroshi Terashima, Yuko Kajiho, Yutaka Harita\",\"doi\":\"10.1111/nep.70069\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Renal angiomyolipomas (AMLs) are a common renal manifestation in tuberous sclerosis complex (TSC), occurring in 50%-85% of cases. Even in asymptomatic individuals, treatment is often initiated based on AML size, with mTOR inhibitors being the primary medical therapy. AMLs tend to enlarge with age, and treatment during school age is rare. Secondary AML shrinkage in paediatric TSC patients has been reported who received everolimus for subependymal giant cell astrocytomas (SEGA) or epilepsy, but studies on its direct use for AMLs in paediatric cases remain limited. A 9-year-old girl born to a mother with TSC was diagnosed at birth due to cardiac rhabdomyomas, cortical tubers, and Shagreen patches. At the age of 4, ultrasound detected multiple AMLs in both kidneys, with the largest lesions measuring 2.3 cm in the right kidney and 1.6 cm in the left. By the age of 7, MRI showed further growth to 4.8 cm. Despite the absence of symptoms, the risk of haemorrhage led to treatment initiation. Everolimus was started at 1.0 mg/day (1.3 mg/m<sup>2</sup>/day), significantly lower than the standard 4.5 mg/m<sup>2</sup>/day. Trough levels remained below the target range, yet AMLs showed a shrinking tendency, with MRI at age 9 revealing a reduction in the largest AML to 2.4 cm. Stomatitis occurred intermittently, but no serious adverse effects were observed. This case suggests that low-dose everolimus can effectively reduce AML size while minimising adverse effects, highlighting its potential as a treatment option for AMLs in paediatric TSC patients.</p>\",\"PeriodicalId\":520716,\"journal\":{\"name\":\"Nephrology (Carlton, Vic.)\",\"volume\":\"30 7\",\"pages\":\"e70069\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12237548/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nephrology (Carlton, Vic.)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1111/nep.70069\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nephrology (Carlton, Vic.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1111/nep.70069","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Successful Treatment of Growing Renal Angiomyolipomas With Low-Dose Everolimus in a School-Aged Child With Tuberous Sclerosis Complex.
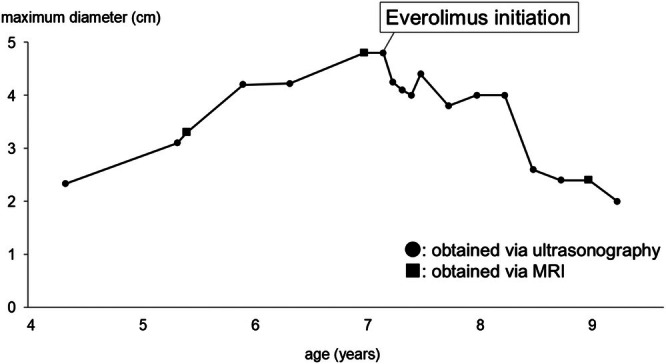
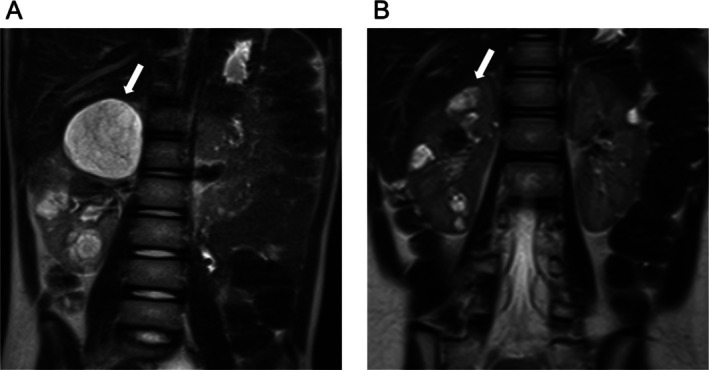
Renal angiomyolipomas (AMLs) are a common renal manifestation in tuberous sclerosis complex (TSC), occurring in 50%-85% of cases. Even in asymptomatic individuals, treatment is often initiated based on AML size, with mTOR inhibitors being the primary medical therapy. AMLs tend to enlarge with age, and treatment during school age is rare. Secondary AML shrinkage in paediatric TSC patients has been reported who received everolimus for subependymal giant cell astrocytomas (SEGA) or epilepsy, but studies on its direct use for AMLs in paediatric cases remain limited. A 9-year-old girl born to a mother with TSC was diagnosed at birth due to cardiac rhabdomyomas, cortical tubers, and Shagreen patches. At the age of 4, ultrasound detected multiple AMLs in both kidneys, with the largest lesions measuring 2.3 cm in the right kidney and 1.6 cm in the left. By the age of 7, MRI showed further growth to 4.8 cm. Despite the absence of symptoms, the risk of haemorrhage led to treatment initiation. Everolimus was started at 1.0 mg/day (1.3 mg/m2/day), significantly lower than the standard 4.5 mg/m2/day. Trough levels remained below the target range, yet AMLs showed a shrinking tendency, with MRI at age 9 revealing a reduction in the largest AML to 2.4 cm. Stomatitis occurred intermittently, but no serious adverse effects were observed. This case suggests that low-dose everolimus can effectively reduce AML size while minimising adverse effects, highlighting its potential as a treatment option for AMLs in paediatric TSC patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


